 Download biomedica product list 2018
Download biomedica product list 2018Bioactive Sclerostin ELISA











-
Category number
BI-20472
-
Method
Sandwich ELISA, HRP/TMB, 12×8-well detachable strips
-
Sample type
Serum, EDTA plasma and citrate plasma
-
Sample volume
20 µl / well
-
Assay time
2 h / 1 h / 30 min
-
Sensitivity
1.9 pmol/l (= 42.7 pg/ml)
-
Standard range
0 – 320 pmol/l (or 0 – 7 200 pg/ml)
-
Precision
In-between-run (n=7): ≤5 % CV
Within-run (n=3): ≤ 1 % CV
-
Regulatory status
Research use only.
-
Validation Data
See validation data tab for: precision, accuracy, diltuion linearity, values for healthy donors, etc.
Product Overview
The bioactive Sclerostin (SOST) immunoassay is a 3.5 hour, 96-well sandwich ELISA for the quantitative determination of bioactive Sclerostin in human serum, EDTA-plasma, and citrate plasma. The assay employs human serum-based standards to ensure the measurement of biologically reliable data.
The human Sclerostin (SOST) immunoassay is an overnight, 96-well sandwich ELISA for the quantitative determination of human Sclerostin in serum, plasma (Citrate, EDTA, Heparin) and urine. The assay employs human serum-based standards to ensure the measurement of biologically reliable data.
The bioactive Sclerostin (SOST) ELISA kit uses highly purified, epitope mapped antibodies with characterized binding kinetics.
The Sclerostin protein (http://www.uniprot.org/uniprot/Q9BQB4.1), a product of the SOST gene, consists of two flexible N- and C-terminal arms and a cystine-knot with three loops, whereas the second loop binds to the LRP5/6 complex of the Wnt-signaling pathway and leads to the inhibition of bone formation (Holdsworth et al., 2012; Veverka et al., 2009).
Sclerostin is classically considered to be a monomeric protein, but data from Hernandez and colleagues (Hernandez et al., 2014) postulate that circulating Sclerostin has a dimeric configuration. Furthermore, it is not yet well understood if circulating Sclerostin fragments exist, but the comparison of different ELISAs suggest that those fragments exist as well (Durosier et al., 2013; Lierop et al., 2010).
As the epitope of the monoclonal capture antibody utilized in the bioactive Sclerostin ELISA is located in loop 2 (see figure below), the binding region to the LRP 5/6 complex, all Sclerostin molecules (including potential fragments) containing this receptor binding region can be detected.
The characterization of both antibodies utilized in the bioactive Sclerostin ELISA comprises epitope mapping with overlapping peptides spotted to a microarray, characterization of binding kinetics with biolayer interferometry measurements and determination of antibody purity with size exclusion chromatography.
Principle of the Assay
The bioactive Sclerostin ELISA kit is a sandwich enzyme immunoassay for the quantitative determination of bioactive Sclerostin (SOST) in human serum and plasma samples.
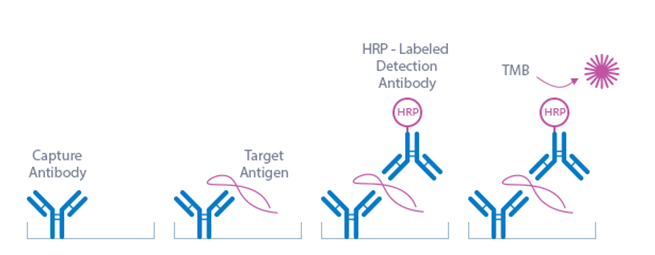
Capture Antibody: recombinant human monoclonal antibody
Detection Antibody: polyclonal goat antibody
Standard: recombinant human bioactive Sclerostin protein (AA24-AA213) in human serum
This kit is a sandwich enzyme immunoassay for the quantitative determination of bioactive sclerostin in human serum and plasma samples (EDTA, citrate). In a first step, assay buffer is pipetted into the wells of the microtiter strips. Thereafter, STD/sample/CTRL are pipetted into the wells, which are pre-coated with the recombinant human monoclonal Sclerostin antibody. Any bioactive Sclerostin present in the STD/sample/CTRL binds to the pre-coated antibody in the well. After incubation, a washing step is applied where all non-specific unbound material is removed. In a next step, the conjugate (anti sclerostin-HRPO) is pipetted into the wells and reacts with bioactive Sclerostin present in the sample, forming a sandwich. After another washing step, the substrate (TMB Tetramethylbenzidine) is pipetted into the wells. The enzyme catalysed colour change of the substrate is directly proportional to the amount of bioactive sclerostin. This colour change is detectable with a standard microtiter plate ELISA reader. A dose response curve of the absorbance (optical density, OD at 450 nm) versus standard concentration is generated, using the values obtained from the standards. The concentration of bioactive sclerostin in the sample is determined directly from the dose response curve.
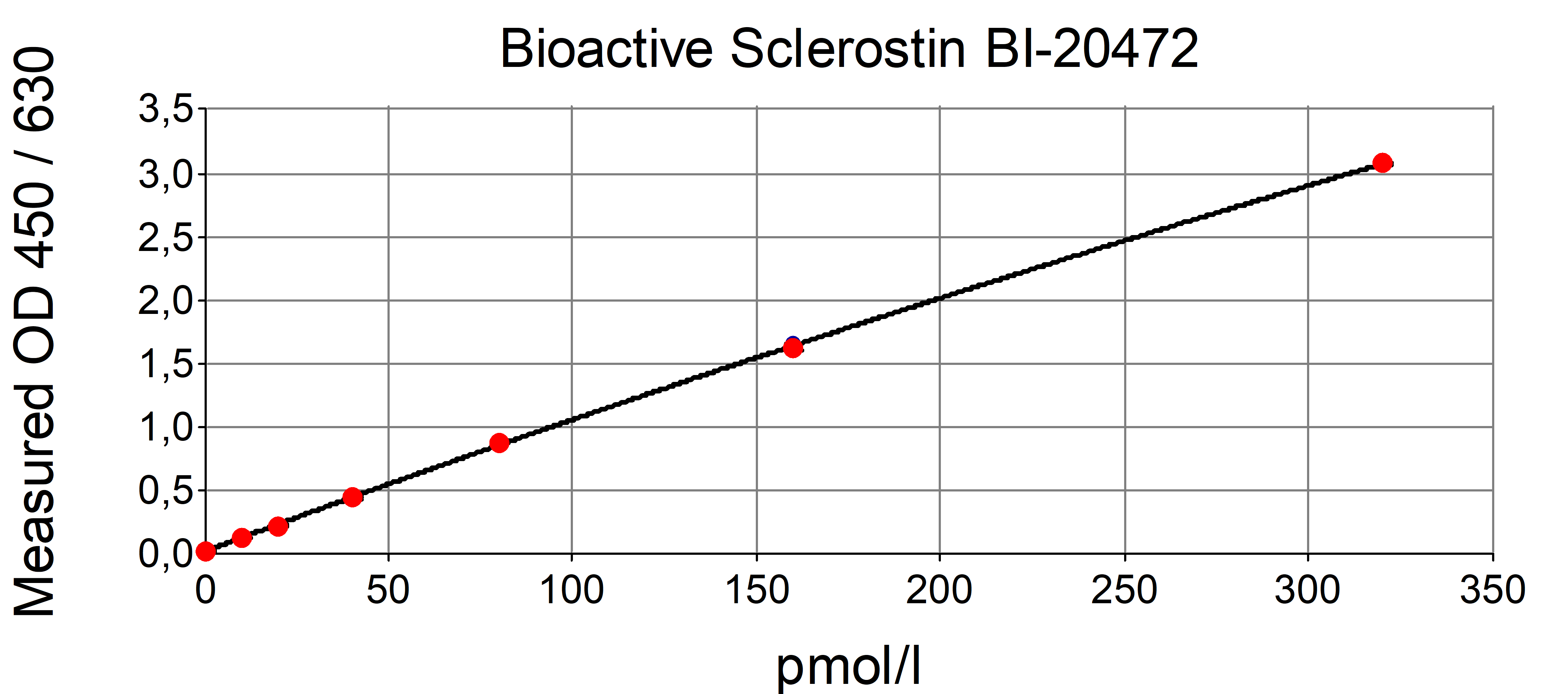
Typical Standard Curve
The figure below shows a typical standard curve for the bioactive Sclerostin (SOST) ELISA. The immunoassay is calibrated against recombinant human bioactive Sclerostin.
Kit Components
|
Contents |
Description |
Quantity |
|
PLATE |
Recombinant human monoclonal Sclerostin antibody, pre-coated microtiter strips in a strip holder, in aluminum bag with desiccant |
12 x 8 tests |
|
WASHBUF |
20 x wash buffer concentrate, natural cap |
1 x 50 ml |
|
ASYBUF |
Assay buffer, red cap, ready to use |
1 x 13 ml |
|
STD |
Standard 1-7 (0; 10; 20; 40; 80; 160; 320 pmol/l), white caps, lyophilized |
7 vials |
|
CTRLS |
Controls A+B, yellow caps, lyophilised (exact concentration on the label) |
2 vials |
|
CONJ |
Conjugate (polyclonal goat anti human Sclerostin antibody)-HRPO, amber bottle, amber cap, ready to use |
1 x 13 ml |
|
SUB |
Substrate (TMB solution), amber bottle, blue cap, ready to use |
1 x 13 ml |
|
STOP |
Stop solution, white cap, ready to use |
1 x 7 ml |
Storage instructions: All reagents of the bioactive Sclerostin ELISA kit are stable at 4°C until the expiry date stated on the label of each reagent.
Serum, EDTA plasma, citrate plasma, cell culture supernatant and urine are suitable for use in this assay. Do not change sample type during studies. We recommend duplicate measurements for all samples, standards and controls. The listed sample collection and storage conditions listed are intended as general guidelines.
Serum & Plasma
Collect venous blood samples in standardized serum separator tubes (SST) or standardized blood collection tubes using EDTA or citrate as an anticoagulant. For serum samples, allow samples to clot for 30 minutes at room temperature. Perform separation by centrifugation according to the tube manufacturer’s instructions for use. Assay the acquired samples immediately or aliquot and store at -25°C or lower. Lipemic or haemolysed samples may give erroneous results. Do not freeze-thaw samples more than five times.
Urine
Note: the experiments performed to measure bioactive Sclerostin in urine samples did not undergo a full validation according to ICH guidelines. However, our performance check suggests that urine samples can be measured with this ELISA. For more information please refer to the validation data.
Aseptically collect the first urine of the day (mid-stream), voided directly into a sterile container. Centrifuge to remove particulate matter, assay immediately or aliquot and store at -25°C or lower.
Cell Culture Supernatant
Note: the experiments performed to measure bioactive Sclerostin in cell culture supernatant samples did not undergo a full validation according to ICH guidelines. However, our performance check suggests that cell culture supernatant samples can be measured with this ELISA. For more information please refer to the validation data.
Remove particulates by centrifugation and assay immediately or aliquot and store samples at -25°C or lower. Do not freeze-thaw samples more than five times.
Reagent Preparation
Wash Buffer
|
1. |
Bring the WASHBUF concentrate to room temperature. Crystals in the buffer concentrate will dissolve at room temperature. |
|
2. |
Dilute the WASHBUF concentrate 1:20, e.g. 50 ml WASHBUF + 950 ml distilled or deionized water. Only use diluted WASHBUF when performing the assay. |
The diluted WASHBUF is stable up to one month at 4°C (2-8°C).
Standards for Serum & Plasma Measurements
|
1. |
Pipette 250 µl of distilled or deionized water into each standard (STDs) and controls (CTRLs) vial. The exact concentration is printed on the label of each vial. |
|
2. |
Leave at room temperature (18-26°C) for 15 min. Vortex gently. |
Reconstituted STDs and CTRLs are stable at -25°C or lower until expiry date stated on the label. STDs and CTRLs are stable for at least 4 freeze-thaw cycles.
Standards for Cell Culture Supernatant Measurements
For the preparation of a cell culture-based standard curve always use the identical cell culture medium (CCM) as used for the experiment.
|
1. |
Reconstitute standard 7 (STD7) in 250 µl deionized water. Leave at room temperature (18-26°C) for 15 min and mix well before making dilutions. Use polypropylene tubes. |
|
2. |
Mark tubes ccSTD6 to ccSTD1. Prepare a twofold serial dilution to obtain STD6 to STD2. e.g. Dispense 100 µl cell culture medium into each vial. |
|
3. |
Pipette 100 µl of STD7 into tube marked as ccSTD6 (containing 100 µl cell culture medium). Mix thoroughly. |
|
4. |
Transfer 100 µl of ccSTD6 into the tube marked as ccSTD5. Mix thoroughly. |
|
5. |
Continue in the same fashion to obtain ccSTD4 to standard 2. CCM serves as the ccSTD1 (0 nmol/l bioactive Sclerostin). |
|
6. |
Using the prepared standards, follow the protocol as indicated for serum samples. |
Attention: Supplied STD1-STD7 and controls are only valid for serum and should not be used for cell culture measurements.
Sample Preparation
Bring samples to room temperature and mix samples gently to ensure the samples are homogenous.
We recommend duplicate measurements for all samples.
Samples with values above STD7 (320 pmol/l) can be diluted with ASYBUF (Assay buffer).
Assay Protocol
Read the entire protocol before beginning the assay.
Bring samples and reagents to room temperature (18-26°C).
Mark positions for STD/SAMPLE/CTRL (Standard/Sample/Control) on the protocol sheet.
|
1. |
Take microtiter strips out of the aluminum bag. Store unused strips with desiccant at 4°C in the aluminum bag. Strips are stable until expiry date stated on the label. |
|
2. |
Pipette 100 µl ASYBUF (assay buffer, red cap) into each well. |
|
3. |
Add 20 µl STD/SAMPLE/CTRL (Standard/Sample/Control) in duplicate into respective well. Swirl gently. |
|
4. |
Cover tightly and incubate for 2 hours at room temperature (18-26°C). |
|
5. |
Aspirate and wash wells 5x with 300 µl diluted WASHBUF (Wash buffer). After final wash, remove remaining WASHBUF by strongly tapping plate against paper towel |
|
6. |
Add 100 µl CONJ (Conjugate, amber cap) into each well. Swirl gently. |
|
7. |
Cover tightly and incubate for 1 hour at room temperature (18-26°C) in the dark. |
|
8. |
Aspirate and wash wells 5x with 300 µl diluted WASHBUF (Wash buffer). After the final wash, remove remaining WASHBUF by strongly tapping plate against paper towel. |
|
9. |
Add 100 µl SUB (Substrate, blue cap) into each well. Swirl gently |
|
10. |
Incubate for 30 min at room temperature (18-26°C) in the dark. |
|
11. |
Add 50 µl STOP (Stop solution, white cap) into each well. Swirl gently |
|
12. |
Measure absorbance immediately at 450 nm with reference 630 nm, if available |
Calculation of Results
Read the optical density (OD) of all wells on a plate reader using 450 nm wavelength (reference wavelength 630 nm). Construct a standard curve from the absorbance read-outs of the standards using commercially available software capable of generating a four-parameter logistic (4-PL) fit. Alternatively, plot the standards’ concentration on the x-axis against the mean absorbance for each standard on the y-axis and draw a best fit curve through the points on the graph. Curve fitting algorithms other than 4-PL have not been validated and will need to be evaluated by the user.
Obtain sample concentrations from the standard curve. If required, pmol/l can be converted into pg/ml by applying a conversion factor (Sclerostin: 1 pg/ml = 0.044 pmol/l, 1 pmol/l = 22.5 pg/ml (MW: 22.5 kDa)). Respective dilution factors must be considered when calculating the final concentration of the sample.
The quality control protocol supplied with the kit shows the results of the final release QC for each kit lot. Data for optical density obtained by customers may differ due to various influences and/or due to the normal decrease of signal intensity during shelf life. However, this does not affect validity of results as long as an OD of 1.50 or more is obtained for the standard with the highest concentration and the values of the CTRLs are in range (target ranges see labels).
INFORMATION ON THE ANALYTE
Sclerostin protein
Sclerostin is a 22.5 kDa secreted glycoprotein that functions as a potent inhibitor of Wnt signaling. Sclerostin is a product of the SOST gene and it acts by binding to the Wnt-coreceptor LRP5/6 thus inhibiting bone formation by regulating osteoblast function and promoting osteoblast apoptosis. The Sclerostin protein consists of two flexible N- and C-terminal arms and a cystine-knot with three loops, whereas the second loop binds to the LRP5/6 complex. Sclerostin is classically considered to be a monomeric protein, but data from Hernandez and colleagues (Hernandez et al., 2014) postulate that circulating sclerostin has a dimeric configuration. In addition, it is not yet well documented if Sclerostin fragments also circulate, but the comparison of different Sclerostin ELISAs suggest that fragments exist as well (Dallas et al., 2013).
|
Molecular Weight |
22.5 kDa |
|
Cellular localization |
Extracellular |
|
Post-translational modifications |
Glycosylation |
|
Sequence similarities |
Sequence similarity to the DAN (differential screening-selected gene aberrative in neuroblastoma) family of bone morphogenetic protein (BMP) antagonists |
|
Alternative Names |
CDD; VBCH; DAND6; SOST1 |
|
Entrez/NCBI ID |
Gene ID: 50964 https://www.ncbi.nlm.nih.gov/gene?Db=gene&Cmd=DetailsSearch&Term=50964 |
|
Genecards |
GC17M043753 link:https://www.genecards.org/cgi-bin/carddisp.pl?gene=SOST |
|
OMIM |
605740 link:https://www.omim.org/entry/605740 |
|
Protein Atlas |
|
|
Uniport ID |
UniProtKB - Q9BQB4 (SOST_HUMAN) https://www.uniprot.org/uniprot/Q9BQB4 |
Sclerostin Function
Sclerostin is nearly exclusively produced in osteocytes (van Bezooijen et al., 2009). Mutations in the Sclerostin (SOST) gene can cause sclerosteosis and van Buchem disease which are bone dysplasia disorders characterized by progressive skeletal overgrowth (Wergedal et al., 2003). Sclerostin levels are altered in response to hormonal stimuli or due to pathophysiological conditions. Sclerostin concentrations are increased in disorders such as hypoparathyroidism (Costa et al., 2011), Paget’s disease (Yavropoulou et al., 2012), multiple myeloma (Terpos et al., 2012) and in cancer induced bone diseases (Yavropoulou et al., 2012). Sclerostin levels are decreased in primary hyperparathyroidism (Lierop et al., 2010), as well as by the mechanical stimulation of bone (Robling et al., 2008). Several studies have found a positive association between sclerostin and bone mineral density (Amrein et al., 2012; Garnero et al., 2013). Sclerostin levels in chronic kidney disease (CKD) patients are increased up to 4-fold compared to patients without CKD and increase with CKD stage and declining kidney function (Cejka et al., 2012; Pelletier et al., 2013). In CKD patients, renal elimination of sclerostin increases with decreasing renal function (Cejka et al., 2014). In dialysis patients, sclerostin is an independent predictor of bone loss (Malluche et al., 2014). Numerous studies have shown that serum sclerostin levels are also associated with cardiovascular events (Kanbay et al., 2014; Viaene et al., 2013). The FDA authorization of a humanized monoclonal Sclerostin antibody for the treatment of osteoporosis in patients at high risk is currently under investigation (McClung, 2017). For reviews please see references (Costa et al., 2017; Drake and Khosla, 2017).
Literature
Sclerostin measurement in human disease: Validity and current limitations.
Costa, A.G., Cremers, S., Bilezikian, J.P., 2017. Bone 96, 24–28.
https://doi.org/10.1016/j.bone.2016.10.012
PMID: 27742501
Hormonal and systemic regulation of sclerostin.
Drake, M.T., Khosla, S., 2017. Bone 96, 8–17.
https://doi.org/10.1016/j.bone.2016.12.004
Clinical utility of anti-sclerostin antibodies.
McClung, M.R., 2017. Bone 96, 3–7.
https://doi.org/10.1016/j.bone.2016.12.012
PMID: 28115281
Renal elimination of sclerostin increases with declining kidney function.
Cejka, D., Marculescu, R., Kozakowski, N., Plischke, M., Reiter, T., Gessl, A., Haas, M., 2014. J. Clin. Endocrinol. Metab. 99, 248–255.
https://doi.org/10.1210/jc.2013-2786
PMID: 24187403
New insights into the location and form of sclerostin.
Hernandez, P., Whitty, C., John Wardale, R., Henson, F.M.D., 2014. Biochem. Biophys. Res. Commun. 446, 1108–1113.
https://doi.org/10.1016/j.bbrc.2014.03.079
PMID: 24667598
Serum sclerostin and adverse outcomes in nondialyzed chronic kidney disease patients.
Kanbay, M., Siriopol, D., Saglam, M., Kurt, Y.G., Gok, M., Cetinkaya, H., Karaman, M., Unal, H.U., Oguz, Y., Sari, S., Eyileten, T., Goldsmith, D., Vural, A., Veisa, G., Covic, A., Yilmaz, M.I., 2014. J. Clin. Endocrinol. Metab. 99, E1854-1861.
https://doi.org/10.1210/jc.2014-2042
PMID: 25057883
Bone Mineral Density and Serum Biochemical Predictors of Bone Loss in Patients with CKD on Dialysis.
Malluche, H.H., Davenport, D.L., Cantor, T., Monier-Faugere, M.-C., 2014. Clin. J. Am. Soc. Nephrol. 9, 1254–1262.
https://doi.org/10.2215/CJN.09470913
The osteocyte: an endocrine cell ... and more.
Dallas, S.L., Prideaux, M., Bonewald, L.F., 2013. Endocr. Rev. 34, 658–690.
https://doi.org/10.1210/er.2012-1026
PMID: 23612223; PMCID: PMC3785641
Association of circulating sclerostin with bone mineral mass, microstructure, and turnover biochemical markers in healthy elderly men and women.
Durosier, C., van Lierop, A., Ferrari, S., Chevalley, T., Papapoulos, S., Rizzoli, R., 2013. J. Clin. Endocrinol. Metab. 98, 3873–3883.
https://doi.org/10.1210/jc.2013-2113
PMID: 23864703
Association of serum sclerostin with bone mineral density, bone turnover, steroid and parathyroid hormones, and fracture risk in postmenopausal women: the OFELY study.
Garnero, P., Sornay-Rendu, E., Munoz, F., Borel, O., Chapurlat, R.D., 2013. Osteoporos. Int. J. Establ. Result Coop. Eur. Found. Osteoporos. Natl. Osteoporos. Found. USA 24, 489–494.
https://doi.org/10.1007/s00198-012-1978-x
PMID: 22525978
The relation between renal function and serum sclerostin in adult patients with CKD.
Pelletier, S., Dubourg, L., Carlier, M.-C., Hadj-Aissa, A., Fouque, D., 2013. Clin. J. Am. Soc. Nephrol. CJASN 8, 819–823.
https://doi.org/10.2215/CJN.07670712
PMID: 23430206; PMCID: PMC3641616
Sclerostin: another bone-related protein related to all-cause mortality in haemodialysis?
Viaene, L., Behets, G.J., Claes, K., Meijers, B., Blocki, F., Brandenburg, V., Evenepoel, P., D’Haese, P.C., 2013. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. - Eur. Ren. Assoc. 28, 3024–3030.
https://doi.org/10.1093/ndt/gft039
PMID: 23605174
Sclerostin and its association with physical activity, age, gender, body composition, and bone mineral content in healthy adults.
Amrein, K., Amrein, S., Drexler, C., Dimai, H.P., Dobnig, H., Pfeifer, K., Tomaschitz, A., Pieber, T.R., Fahrleitner-Pammer, A., 2012. J. Clin. Endocrinol. Metab. 97, 148–154.
https://doi.org/10.1210/jc.2011-2152
PMID: 21994959
Sclerostin serum levels correlate positively with bone mineral density and microarchitecture in haemodialysis patients.
Cejka, D., Jager-Lansky, A., Kieweg, H., Weber, M., Bieglmayer, C., Haider, D.G., Diarra, D., Patsch, J.M., Kainberger, F., Bohle, B., Haas, M., 2012. Nephrol. Dial. Transplant. 27, 226–230.
https://doi.org/10.1093/ndt/gfr270
Characterization of the interaction of sclerostin with the low density lipoprotein receptor-related protein (LRP) family of Wnt co-receptors.
Holdsworth, G., Slocombe, P., Doyle, C., Sweeney, B., Veverka, V., Le Riche, K., Franklin, R.J., Compson, J., Brookings, D., Turner, J., Kennedy, J., Garlish, R., Shi, J., Newnham, L., McMillan, D., Muzylak, M., Carr, M.D., Henry, A.J., Ceska, T., Robinson, M.K., 2012. J. Biol. Chem. 287, 26464–26477.
https://doi.org/10.1074/jbc.M112.350108
PMID: 22696217; PMCID: PMC3410989
Elevated circulating sclerostin correlates with advanced disease features and abnormal bone remodeling in symptomatic myeloma: reduction post-bortezomib monotherapy.
Terpos, E., Christoulas, D., Katodritou, E., Bratengeier, C., Gkotzamanidou, M., Michalis, E., Delimpasi, S., Pouli, A., Meletis, J., Kastritis, E., Zervas, K., Dimopoulos, M.A., 2012. Int. J. Cancer 131, 1466–1471.
https://doi.org/10.1002/ijc.27342
PMID: 22052418
Serum sclerostin levels in Paget’s disease and prostate cancer with bone metastases with a wide range of bone turnover.
Yavropoulou, M.P., van Lierop, A.H., Hamdy, N.A.T., Rizzoli, R., Papapoulos, S.E., 2012. Bone 51, 153–157.
https://doi.org/10.1016/j.bone.2012.04.016
PMID: 22579776
Circulating Sclerostin in Disorders of Parathyroid Gland Function.
Costa, A.G., Cremers, S., Rubin, M.R., McMahon, D.J., Sliney, J., Lazaretti-Castro, M., Silverberg, S.J., Bilezikian, J.P., 2011. J. Clin. Endocrinol. Metab. 96, 3804–3810.
https://doi.org/10.1210/jc.2011-0566
PMID: 21937621; PMCID: PMC3232608
Determination of serum and plasma sclerostin concentrations by enzyme-linked immunoassays.
McNulty, M., Singh, R.J., Li, X., Bergstralh, E.J., Kumar, R., 2011. J. Clin. Endocrinol. Metab. 96, E1159-1162.
https://doi.org/10.1210/jc.2011-0254
PMID: 21543425; PMCID: PMC3135202
Patients with primary hyperparathyroidism have lower circulating sclerostin levels than euparathyroid controls.
Lierop, A.H. van, Witteveen, J.E., Hamdy, N. a. T., Papapoulos, S.E., 2010. Eur. J. Endocrinol. 163, 833–837.
https://doi.org/10.1530/EJE-10-0699
Sclerostin in mineralized matrices and van Buchem disease.
van Bezooijen, R.L., Bronckers, A.L., Gortzak, R.A., Hogendoorn, P.C.W., van der Wee-Pals, L., Balemans, W., Oostenbroek, H.J., Van Hul, W., Hamersma, H., Dikkers, F.G., Hamdy, N. a. T., Papapoulos, S.E., Löwik, C.W.G.M., 2009. J. Dent. Res. 88, 569–574.
https://doi.org/10.1177/0022034509338340
PMID: 19587164
Characterization of the structural features and interactions of sclerostin: molecular insight into a key regulator of Wnt-mediated bone formation.
Veverka, V., Henry, A.J., Slocombe, P.M., Ventom, A., Mulloy, B., Muskett, F.W., Muzylak, M., Greenslade, K., Moore, A., Zhang, L., Gong, J., Qian, X., Paszty, C., Taylor, R.J., Robinson, M.K., Carr, M.D., 2009. J. Biol. Chem. 284, 10890–10900.
https://doi.org/10.1074/jbc.M807994200
PMID: 19208630; PMCID: PMC2667775
Mechanical stimulation of bone in vivo reduces osteocyte expression of Sost/sclerostin.
Robling, A.G., Niziolek, P.J., Baldridge, L.A., Condon, K.W., Allen, M.R., Alam, I., Mantila, S.M., Gluhak-Heinrich, J., Bellido, T.M., Harris, S.E., Turner, C.H., 2008. J. Biol. Chem. 283, 5866–5875.
https://doi.org/10.1074/jbc.M705092200
PMID: 18089564
Patients with Van Buchem disease, an osteosclerotic genetic disease, have elevated bone formation markers, higher bone density, and greater derived polar moment of inertia than normal.
Wergedal, J.E., Veskovic, K., Hellan, M., Nyght, C., Balemans, W., Libanati, C., Vanhoenacker, F.M., Tan, J., Baylink, D.J., Van Hul, W., 2003. J. Clin. Endocrinol. Metab. 88, 5778–5783.
https://doi.org/10.1210/jc.2003-030201
PMID: 14671168
All Biomedica ELISAs are validated according to international FDA/ICH/EMEA guidelines. For more information about our validation guidelines, please refer to our quality page and published validation guidelines and literature.
Validation literature
- ICH Q2(R1) Validation of Analytical Procedures: Text and Methodology.
- EMEA/CHMP/EWP/192217/2009 Guideline on bioanalytical method validation.
- Bioanalytical Method Validation, Guidance for Industry, FDA, May 2018
Calibration
The bioactive Sclerostin immunoassay is calibrated against recombinant bioactive Sclerostin protein UniProtKB - Q9BQB4 (SOST_HUMAN) https://www.uniprot.org/uniprot/Q9BQB4.
Detection Limit & Sensitivity
To determine the sensitivity of the bioactive Sclerostin ELISA, experiments measuring the Lower Limit of Detection (LOD) and the Lower Limit of Quantification (LLOQ) were conducted.
The LOD, also called the detection limit, is the lowest point at which a signal can be distinguished above the background signal, i.e. the signal that is measured in the absence of bioactive Sclerostin, with a confidence level of 99%. It is defined as the mean back calculated concentration of standard 1 (0 pmol/l of bioactive Sclerostin, five independent measurements) plus three times the standard deviation of the measurements.
The LLOQ, or sensitivity of an assay, is the lowest concentration at which an analyte can be accurately quantified. The criteria for accurate quantification at the LLOQ are an analyte recovery between 75 and 125% and a coefficient of variation (CV) of less than 25%. To determine the LLOQ, standard 2, i.e. the lowest standard containing bioactive Sclerostin, is diluted, measured five times and its concentration is back calculated. The lowest dilution, which meets both criteria, is reported as the LLOQ.
The following values were determined for the bioactive Sclerostin ELISA:
|
LOD |
1.9 pmol/l |
|
LLOQ |
1.3 pmol/l |
Precision
The precision of an ELISA is defined as its ability to measure the same concentration consistently within the same experiments carried out by one operator (within-run precision or repeatability) and across several experiments using the same samples but conducted by several operators at different locations using different ELISA lots (in-between-run precision or reproducibility).
Within-Run Precision
Within-run / intra-assay precision was assessed by measuring two samples of known concentrations three times within one bioactive Sclerostin ELISA lot by one operator.
|
ID |
n |
Mean bioactive Sclerostin [pmol/l] |
SD [pmol/l] |
CV (%) |
|
Sample 1 |
3 |
19 |
0.3 |
1 |
|
Sample 2 |
3 |
153 |
1.0 |
1 |
In-Between-Run Precision
In-between-run precision / intra-assay precision was assessed by measuring two samples seven times within two bioactive Sclerostin ELISA lots by two operators.
|
ID |
n |
Mean bioactive Sclerostin [pmol/l] |
SD [pmol/l] |
CV (%) |
|
Sample 1 |
7 |
19 |
1.0 |
5 |
|
Sample 2 |
7 |
157 |
8.3 |
5 |
Accuracy
The accuracy of an ELISA is defined as the precision with which it can recover samples of known concentrations.
The recovery of the bioactive SclerostinELISA was measured by adding recombinant bioactive Sclerostin to clinical samples containing a known concentration endogenous bioactive Sclerostin. The %recovery of the spiked concentration was calculated as the percentage of measured compared over the expected value. All our ELISAs are expected to have %recovery rates within 15% of the nominal value of the sample.
This table shows the summary of the recovery experiments in the bioactive Sclerostin ELISA in different matrices:
|
|
% Recovery |
||||
|
Sample Matrix |
n |
+ 26 pmol/l |
+ 110 pmol/l |
||
|
Mean |
Range |
Mean |
Range |
||
|
Serum |
5 |
93% |
76-111% |
86% |
82-95% |
|
EDTA plasma |
5 |
94% |
85-104% |
93% |
86-98% |
|
Citrate plasma |
1 |
104% |
- |
99% |
- |
Experiments:
Recovery of spiked samples was tested by adding 2 concentrations of human recombinant bioactive Sclerostin (26 pmol/l + 110 pmol/l) to different human sample matrices.
Data showing spike/recovery of human serum samples:
|
|
bioactive Sclerostin [pmol/l] |
Recovery (%) |
|||
|
Sample ID |
Reference |
+26 pmol/l |
+110 pmol/l |
+26 pmol/l |
+110 pmol/l |
|
#S1 |
57 |
77 |
147 |
76 |
82 |
|
#S2 |
75 |
104 |
180 |
111 |
95 |
|
#S3 |
55 |
77 |
148 |
84 |
84 |
|
#S4 |
44 |
67 |
140 |
90 |
87 |
|
#S5 |
71 |
97 |
164 |
101 |
84 |
|
Mean |
93 |
86 |
|||
Data showing spike/recovery of human EDTA plasma samples:
|
|
bioactive Sclerostin [pmol/l] |
Recovery (%) |
|||
|
Sample ID |
Reference |
+26 pmol/l |
+110 pmol/l |
+26 pmol/l |
+110 pmol/l |
|
#E1 |
190 |
212 |
295 |
85 |
96 |
|
#E2 |
152 |
177 |
253 |
95 |
92 |
|
#E3 |
165 |
190 |
259 |
97 |
86 |
|
#E4 |
81 |
108 |
189 |
104 |
98 |
|
#E5 |
67 |
91 |
171 |
91 |
94 |
|
Mean |
94 |
93 |
|||
Data showing spike/recovery of human citrate plasma samples:
|
|
bioactive Sclerostin [pmol/l] |
Recovery (%) |
|||
|
Sample ID |
Reference |
+26 pmol/l |
+110 pmol/l |
+26 pmol/l |
+110 pmol/l |
|
#C1 |
90 |
117 |
199 |
104 |
99 |
Dilution Linearity & Parallelism
Tests of dilution linearity and parallelism ensure that both endogenous and recombinant samples containing bioactive Sclerostin behave in a dose dependent manner and are not affected by matrix effects. Dilution linearity assesses the accuracy of measurements in diluted clinical samples spiked with known concentrations of recombinant analyte. By contrast, parallelism refers to dilution linearity in clinical samples and provides evidence that the endogenous analyte behaves in same way as the recombinant one. Dilution linearity and parallelism are assessed for each sample type and are considered acceptable if the results are within ± 20% of the expected concentration.
Dilution linearity was assessed by serially diluting samples spiked with 110 pmol/l recombinant bioactive Sclerostin with assay buffer.
The table below show the mean recovery and range of serially diluted recombinant bioactive Sclerostin in several sample matrices:
|
|
|
% Recovery of recombinant bioactive Sclerostin in diluted samples |
|||||||
|
Sample Matrix |
n |
1+1 |
1+3 |
1+7 |
1+15 |
||||
|
Mean |
Range |
Mean |
Range |
Mean |
Range |
Mean |
Range |
||
|
Serum |
6 |
98 |
93-103 |
86 |
73-100 |
89 |
75-103 |
98 |
93-103 |
|
EDTA plasma |
6 |
102 |
97-106 |
99 |
97-103 |
91 |
91-109 |
102 |
97-106 |
|
Citrate plasma |
1 |
119 |
- |
132 |
- |
103 |
- |
119 |
- |
All samples were diluted in assay buffer provided in the kit.
Data showing dilution linearity of 110 pmol/l recombinant bioactive Sclerostin spiked into
human blood samples (reference) containing endogenous bioactive Sclerostin.
Serum samples:
|
Sample ID |
bioactive Sclerostin [pmol/l] |
Recovery (%) |
|||||
|
Reference |
1+1 |
1+3 |
1+7 |
1+1 |
1+3 |
1+7 |
|
|
#S1 |
147 |
71 |
37 |
17 |
96 |
100 |
93 |
|
#S2 |
180 |
84 |
37 |
19 |
93 |
82 |
83 |
|
#S3 |
259 |
134 |
62 |
27 |
103 |
96 |
82 |
|
#S4 |
148 |
76 |
31 |
19 |
103 |
85 |
100 |
|
#S5 |
140 |
67 |
27 |
18 |
96 |
78 |
103 |
|
#S6 |
164 |
78 |
30 |
15 |
95 |
73 |
75 |
|
|
|
|
|
Mean R [%] |
98 |
86 |
89 |
EDTA plasma samples:
|
Sample ID |
bioactive Sclerostin [pmol/l] |
R [%] |
|||||
|
Reference |
1+1 |
1+3 |
1+7 |
1+1 |
1+3 |
1+7 |
|
|
#E1 |
295 |
151 |
72 |
35 |
102 |
97 |
96 |
|
#E2 |
184 |
91 |
45 |
21 |
99 |
98 |
93 |
|
#E3 |
253 |
128 |
62 |
29 |
101 |
97 |
91 |
|
#E4 |
259 |
136 |
67 |
32 |
105 |
103 |
97 |
|
#E5 |
189 |
101 |
46 |
22 |
106 |
97 |
95 |
|
#E6 |
171 |
83 |
44 |
23 |
97 |
103 |
109 |
|
|
|
|
|
Mean R [%] |
102 |
99 |
97 |
|
Sample ID |
bioactive Sclerostin [pmol/l] |
R [%] |
|||||
|
Reference |
1+1 |
1+3 |
1+7 |
1+1 |
1+3 |
1+7 |
|
|
#C1 |
174 |
103 |
58 |
22 |
119 |
132 |
103 |
Parallelism was assessed by serially diluting samples containing endogenous bioactive Sclerostin with assay buffer.
The table below shows the mean recovery and range of serially diluted endogenous bioactive Sclerostin in several sample matrices:
|
Matrix |
Recovery of dilution steps (%) |
|||||
|
1+1 |
1+3 |
1+7 |
||||
|
Mean |
Range |
Mean |
Range |
Mean |
Range |
|
|
Serum (n=7) |
100 |
89-108 |
103 |
96-108 |
106 |
90-120 |
|
EDTA plasma (n=6) |
105 |
99-111 |
108 |
99-125 |
123 |
107-154 |
|
Citrate plasma (n=2) |
91 |
89-94 |
91 |
86-96 |
103 |
102-104 |
All samples were diluted in assay buffer provided in the kit.
Data showing the dilution of endogenous bioactive Sclerostin in serum samples:
|
1+7 |
1+7 |
||||||
|
#S1 |
139 |
67 |
33 |
17 |
97 |
96 |
95 |
|
#S2 |
122 |
60 |
33 |
18 |
98 |
108 |
120 |
|
#S3 |
114 |
61 |
29 |
13 |
108 |
101 |
90 |
|
#S4 |
139 |
75 |
39 |
20 |
108 |
112 |
116 |
|
#S5 |
103 |
50 |
28 |
15 |
98 |
108 |
116 |
|
#S6 |
199 |
88 |
48 |
25 |
89 |
96 |
101 |
|
#S7 |
89 |
46 |
23 |
12 |
104 |
105 |
106 |
|
|
|
|
|
Mean |
100 |
103 |
106 |
Data showing the dilution of endogenous bioactive Sclerostin in EDTA plasma samples:
|
Sample ID |
bioactive Sclerostin [pmol/l] |
Recovery (%) |
|||||
|
Reference |
1+1 |
1+3 |
1+7 |
1+1 |
1+3 |
1+7 |
|
|
#E1 |
268 |
147 |
66 |
36 |
110 |
99 |
107 |
|
#E2 |
210 |
109 |
52 |
30 |
104 |
99 |
115 |
|
#E3 |
173 |
87 |
50 |
28 |
100 |
116 |
131 |
|
#E4 |
184 |
98 |
47 |
28 |
106 |
102 |
122 |
|
#E5 |
148 |
82 |
46 |
28 |
111 |
125 |
154 |
|
#E6 |
242 |
120 |
66 |
32 |
99 |
110 |
107 |
|
|
|
|
|
Mean |
105 |
108 |
123 |
Data showing the dilution of endogenous bioactive Sclerostin in citrate plasma samples:
|
Sample ID |
bioactive Sclerostin [pmol/l] |
Recovery (%) |
|||||
|
Reference |
1+1 |
1+3 |
1+7 |
1+1 |
1+3 |
1+7 |
|
|
#C1 |
175 |
82 |
42 |
23 |
94 |
96 |
104 |
|
#C2 |
171 |
76 |
37 |
22 |
89 |
86 |
102 |
|
|
|
|
|
Mean |
91 |
91 |
103 |
Experiment:
Dilution linearity was assessed by serially diluting samples containing 110 pmol/l recombinant bioactive Sclerostin with assay buffer.
Data showing the dilution of recombinant bioactive Sclerostin in serum samples:
|
Sample ID |
bioactive Sclerostin [pmol/l] |
Recovery (%) |
|||||
|
Reference |
1+1 |
1+3 |
1+7 |
1+1 |
1+3 |
1+7 |
|
|
#S1 |
147 |
71 |
37 |
17 |
96 |
100 |
93 |
|
#S2 |
180 |
84 |
37 |
19 |
93 |
82 |
83 |
|
#S3 |
259 |
134 |
62 |
27 |
103 |
96 |
82 |
|
#S4 |
148 |
76 |
31 |
19 |
103 |
85 |
100 |
|
#S5 |
140 |
67 |
27 |
18 |
96 |
78 |
103 |
|
#S6 |
164 |
78 |
30 |
15 |
95 |
73 |
75 |
|
|
|
|
|
Mean |
98 |
86 |
89 |
Data showing the dilution of recombinant bioactive Sclerostin in EDTA plasma samples:
|
Sample ID |
bioactive Sclerostin [pmol/l] |
Recovery (%) |
|||||
|
Reference |
1+1 |
1+3 |
1+7 |
1+1 |
1+3 |
1+7 |
|
|
#E1 |
295 |
151 |
72 |
35 |
102 |
97 |
96 |
|
#E2 |
184 |
91 |
45 |
21 |
99 |
98 |
93 |
|
#E3 |
253 |
128 |
62 |
29 |
101 |
97 |
91 |
|
#E4 |
259 |
136 |
67 |
32 |
105 |
103 |
97 |
|
#E5 |
189 |
101 |
46 |
22 |
106 |
97 |
95 |
|
#E6 |
171 |
83 |
44 |
23 |
97 |
103 |
109 |
|
|
|
|
|
Mean |
102 |
99 |
97 |
Data showing the dilution of recombinant bioactive Sclerostin in citrate plasma samples:
|
Sample ID |
bioactive Sclerostin [pmol/l] |
R [%] |
|||||
|
Reference |
1+1 |
1+3 |
1+7 |
1+1 |
1+3 |
1+7 |
|
|
#C1 |
174 |
103 |
58 |
22 |
119 |
132 |
103 |
Specificity
The specificity of an ELISA is defined as its ability to exclusively recognize the analyte of interest.
The specificity of the bioactive Sclerostin ELISA was shown by characterizing both the capture and the detection antibody through epitope mapping with overlapping peptides spotted to a microarray, characterization of binding kinetics with biolayer interferometry measurements and determination of antibody purity with size exclusion chromatography and affinity measurements. In addition, the specificity of the ELISA was established through competition experiments, which measure the ability of the antibodies to exclusively bind bioactive Sclerostin.
Epitope Mapping
Antibody binding sites were determined by epitope mapping using microarray analysis (Pepperprint GmbH).

Sclerostin Protein Structure - EPITOPES OF COATING AND DETECTION ANTIBODY
Affinities of Coating and Detection Antibodies
Antibody affinities to bioactive Sclerostin were tested by biolayer interferometry measurements (Octet), which measures the binding of antibodies to a bioactive Sclerostin coated sensor.
The results of these measurements are shown in the figure below.
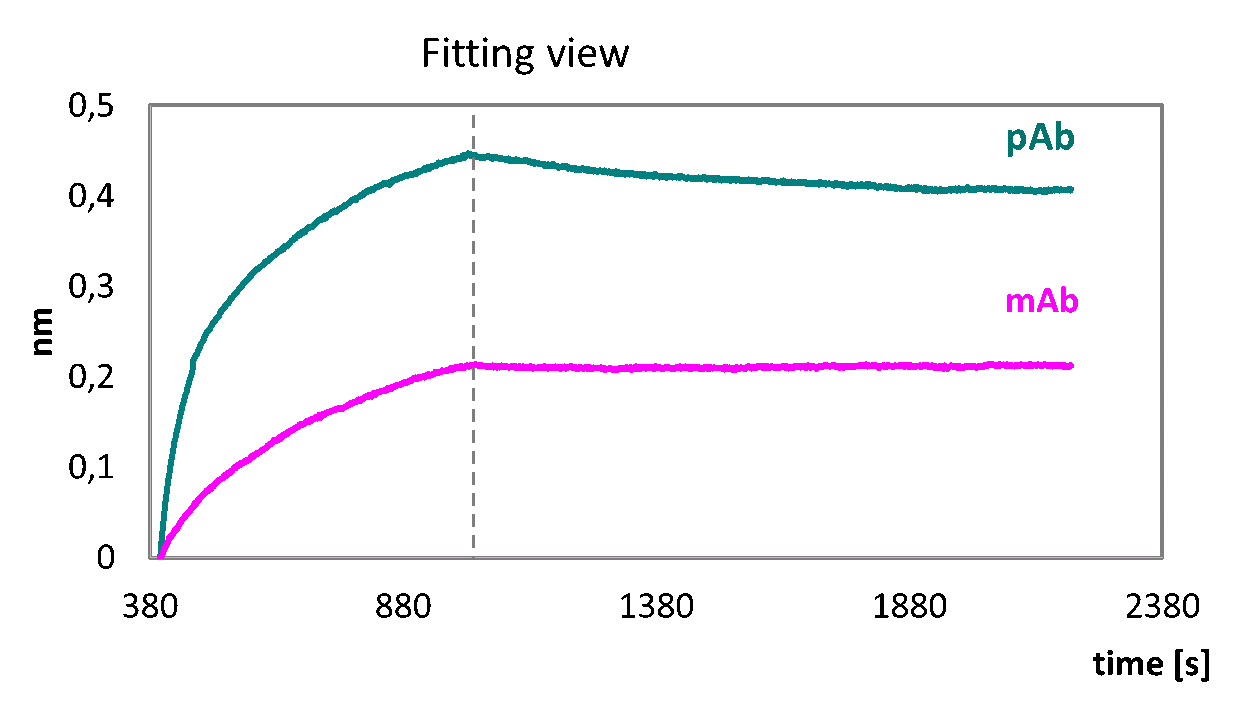
Both ELISA antibodies utilized in the “bioactive Sclerostin ELISA” bind to Sclerostin with high affinity.
Biolayer interferometry measurements (Octet) of monoclonal coating antibody (mAb, pink) and polyclonal detection antibody (pAb, turquoise) binding to a sensor coated with sclerostin protein.
Both antibodies used in the bioactive Sclerostin ELISA bind to bioactive Sclerostin with high affinity.
Antibody Purity
Both the coating and detection antibodies were purified by HPLC. The figures below reveal the high purity (>95%) of the antibody monomers used in the bioactive Sclerostin ELISA.
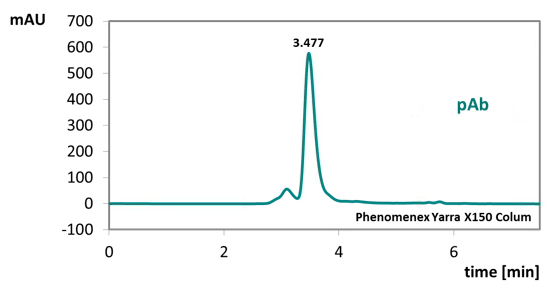
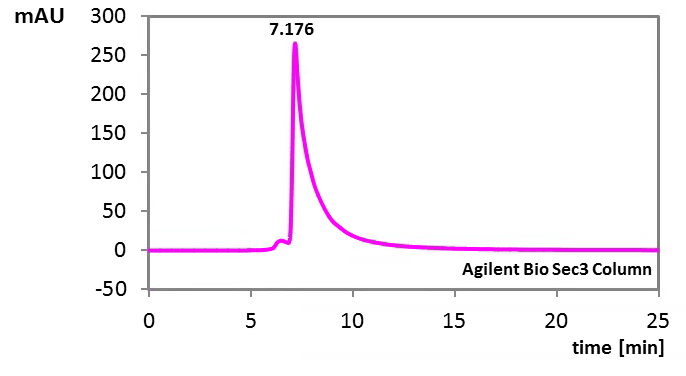
HPLC analysis of both antibodies. Size exclusion chromatography (SEC) of monoclonal antibody (mAb, pink) and polyclonal antibody (pAb, turquoise). The monoclonal antibody was analyzed using an Agilent Bio Sec column, whereas for the polyclonal antibody a Phenomenex Yarra X150 column was used.
Competition of Signal
Competition experiments were carried out by pre-incubating human samples, containing endogenous concentrations of human bioactive Sclerostin, with an excess of coating antibody. The concentration measured in this mixture was then compared to a reference value, which was obtained from the same sample but without the pre-incubation step.
|
Bioactive Sclerostin [pmol/l] |
% Competition |
|||
|
Sample matrix |
ID |
Reference |
Reference + capture AB |
|
|
Serum |
s1 |
28 |
28 |
100 |
|
Serum |
s2 |
39 |
39 |
100 |
|
EDTA plasma |
e1 |
40 |
40 |
100 |
|
EDTA plasma |
e2 |
245 |
245 |
100 |
|
EDTA plasma |
e3 |
88 |
88 |
100 |
|
Citrate plasma |
c1 |
112 |
112 |
100 |
|
Citrate plasma |
c2 |
108 |
108 |
99 |
|
Mean |
100 |
|||
Sample Stability
The stability of endogenous bioactive Sclerostin was tested by comparing measurements in samples that had undergone up to four freeze-thaw cycles.
For freeze-thaw experiments, samples were collected according to the supplier’s instruction using blood collection devices and stored at -80°C.
A set of samples (3 sera, 3 EDTA plasma, 2 citrate plasma) was aliquoted and freeze-thaw stressed. The reference samples are freeze thawed once. Samples can undergo 4 freeze-thaw cycles. The mean recovery of sample concentrations stressed by 4 freeze-thaw cycles is 93%.
Bioactive Sclerostin concentrations of samples after freeze-thaw cycles:
|
|
bioactive Sclerostin [pmol/l] |
Recovery (%) 4 F/T vs ref |
|||
|
Sample ID |
Reference |
2x |
3x |
4x |
|
|
#s1 |
27 |
22 |
25 |
29 |
109 |
|
#s2 |
40 |
35 |
33 |
35 |
87 |
|
#s3 |
42 |
38 |
41 |
40 |
94 |
|
#e1 |
236 |
224 |
231 |
226 |
96 |
|
#e2 |
108 |
90 |
95 |
98 |
90 |
|
#e3 |
98 |
85 |
91 |
91 |
93 |
|
#c1 |
114 |
99 |
101 |
99 |
86 |
|
#c2 |
114 |
108 |
100 |
100 |
88 |
|
Mean |
93 |
||||
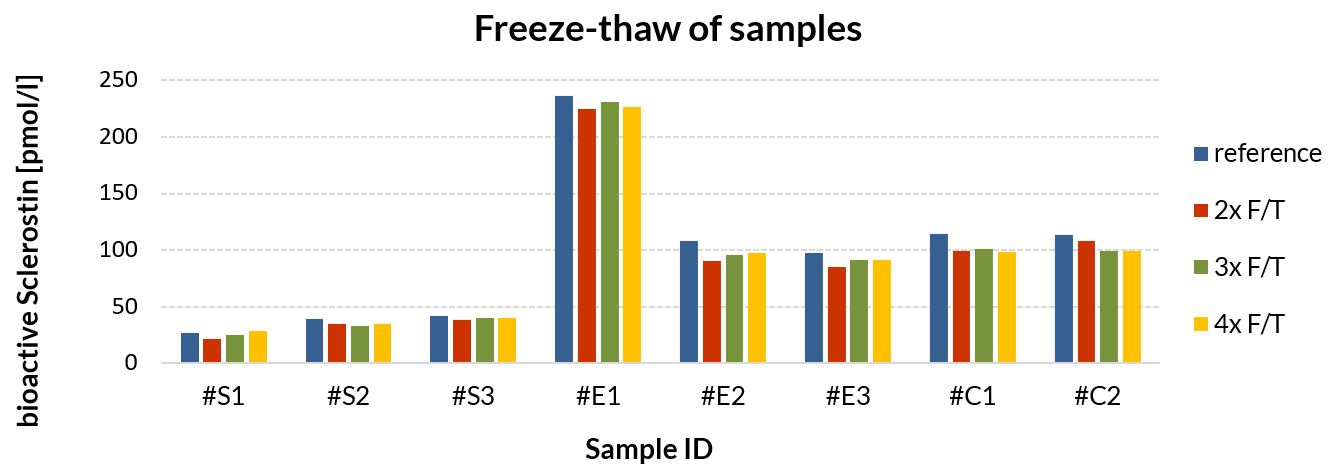
Samples can undergo at least up to 4 freeze-thaw cycles.
Sample Values
Bioactive Sclerostin Values in Apparently Healthy Individuals
To provide expected values for circulating bioactive Sclerostin, a panel of samples from apparently healthy donors was tested.
A summary of the results is shown below:
|
|
Bioactive Sclerostin [pmol/l] |
||||||
|
Sample Matrix |
n |
Mean |
Median |
5% Percentile |
95% Percentile |
Minimum |
Maximum |
|
Serum |
32 |
70.8 |
61.5 |
12.5 |
143.4 |
8 |
183 |
|
EDTA plasma |
24 |
103.9 |
87 |
29.2 |
225.8 |
27 |
235 |
|
Citrate plasma |
24 |
72.8 |
61.5 |
19.2 |
165.3 |
18 |
166 |
It is recommended to establish the normal range for each laboratory.
Plasma Bioactive Sclerostin Values in Kidney Transplant Recipients
|
|
Bioactive Sclerostin [pmol/l] |
||||||
|
Sample Matrix |
n |
Mean |
Median |
5% Percentile |
95% Percentile |
Minimum |
Maximum |
|
EDTA plasma |
16 |
170.3 |
166.5 |
71 |
310 |
71 |
310 |
![]()
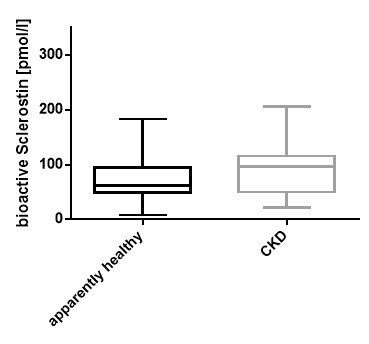
Serum Bioactive Sclerostin Values in a CKD Patient Cohort
|
|
Apparently Healthy Subjects |
CKD |
|
|
||
|
n |
32 |
24 |
|
Mean |
70.8 |
94.1 |
|
Median |
61.5 |
96 |
|
Percentile 95% |
143.4 |
200.3 |
|
Percentile 5% |
12.5 |
22.7 |
|
Minimum |
8 |
21 |
|
Maximum |
183 |
206 |
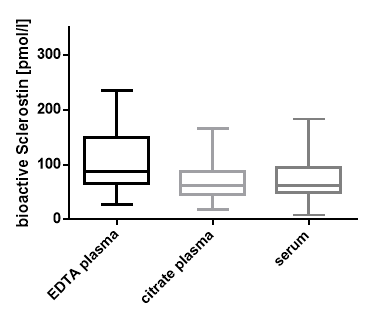
Matrix Comparision
To assess whether all tested matrices behave the same way in the bioactive Sclerostin ELISA, concentrations of bioactive Sclerostin were measured in serum, EDTA, and citrate plasma samples prepared from six apparently healthy donors. Each individual donated blood in all tested sample matrices.
A summary table of bioactive Sclerostin levels in various sample matrices is shown below:
|
|
bioactive Sclerostin [pmol/l] |
|||
|
Donor ID |
EDTA plasma |
Citrate plasma |
Serum |
|
|
#1 |
89 |
74 |
57 |
|
|
#2 |
27 |
23 |
15 |
|
|
#3 |
65 |
43 |
39 |
|
|
#4 |
66 |
58 |
56 |
|
|
#5 |
66 |
57 |
56 |
|
|
#6 |
60 |
54 |
52 |
|
Measured values of human bioactive Sclerostin in serum are lower compared to plasma in an apparently healthy cohort (n=6).
It has been shown that Sclerostin values differ between serum and plasma even when these assays are validated in both matrices (McNulty et al., 2011). Measurements of Sclerostin in plasma are generally higher than in serum. The reasons for this difference are still unclear, however it is assumed that coagulation process under conditions of serum collection might reduce the accessibility of recognizable determinants (Costa et al., 2017).

Figure showing matrix comparison of bioactive Sclerostin sample concentrations between serum, EDTA plasma, and citrate plasma in an apparently healthy cohort (n=6).
Why is heparin plasma not suggested as a sample matrix in this ELISA?
Heparin mainly binds on loop2 and loop3 of the Sclerostin molecule.
Heparin disturbs the binding of the detection antibody utilized in this ELISA assay. For this reason, heparin-plasma cannot be measured with this assay.
Comparison with other Assays
Biomedica’s Sclerostin ELISA (cat.no. BI-20492*) was compared with the bioactive Sclerostin ELISA (cat.no. BI-20472**). The same panel of samples was tested (16 EDTA plasma samples and 16 serum samples). The correlation between the two assays was R= 0.58.
*launched 2013, ** launched 2018
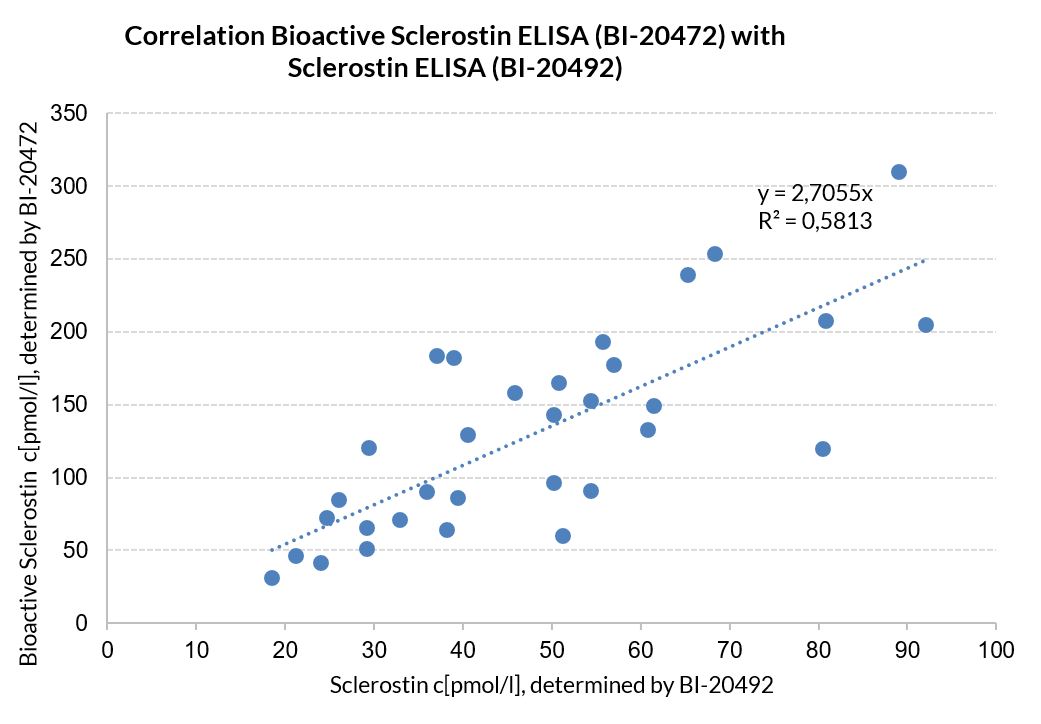
Results: The correlation between the two assays resulted in R2=0.58. Sclerostin sample values measured with the Biomedica “bioactive Sclerostin ELISA” (cat no BI-20472) are higher than in the Biomedica “Sclerostin ELISA” (cat no BI-20492). The results demonstrate that the antibodies utilized in both assays bind to different regions of the Sclerostin molecule. The monoclonal capture antibody of the bioactive Sclerostin ELISA binds to the receptor binding site of Sclerostin; a region that is most probably more robust to cleavage.
Increased bioactive sclerostin levels in kidney transplant recipients detected with a new and well-characterized ELISA (ISN Frontiers Tokyo Feb 2018 - #P-300)
