 Download biomedica product list 2018
Download biomedica product list 2018NT-proANP ELISA





-
Category number
BI-20892
-
Method
Sandwich ELISA, HRP/TMB, 12×8-well detachable strips
-
Sample type
Serum, EDTA plasma, citrate plasma, heparin plasma, urine, cell culture supernatant
-
Sample volume
10 µl / well
-
Assay time
3 h / 30 min
-
Sensitivity
0.05 nmol/l (= 0.64 ng/ml)
-
Standard range
0 – 10 nmol/l (= 0 – 127 ng/ml)
-
Conversion factor
1 nmol/l = 12.7 ng/ml (MW: 12.7 kDa)
-
Precision
In-between-run (n=3): ≤ 9 % CV
Within-run (n=5): ≤ 5 % CV
-
Cross-reactivity
proANP (1-30) <1%, proANP (31-67) <1%, proANP (79-98) <1%, alpha ANP (99-126)<1%
proBNP (8-29) <1%, proBNP (32-57) <1%
proCNP (1-19) <1%, proCNP (30-50) <1%, proCNP (51-97) <1%
The assay also detects mouse and rat proANP (1-98).
-
Validation Data
See validation data tab for: precision, accuracy, diltuion linearity, values for healthy donors, etc.
Product Overview
The NT-proANP immunoassay* is a 3.5 hour, 96-well sandwich ELISA for the quantitative determination of NT-proANP in human serum, EDTA plasma, heparin plasma, cell culture supernatants and urine.
*Please note that the name of this assay has been changed from proANP (1-98) ELISA to NT-proANP ELISA, referring to a more recent terminology for the peptide.
Principle of the Assay
This kit is a sandwich enzyme immunoassay for the quantitative determination of NT-proANP in human serum, EDTA plasma, heparin plasma, cell culture supernatants and urine. The assay has also been validated for rat samples.
The figure below explains the principle of a sandwich ELISA:
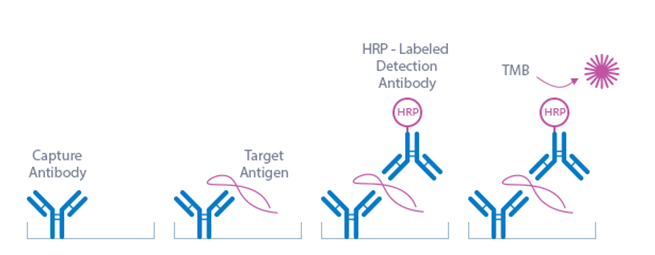
In a first step, sample and conjugate (sheep anti-human NT-proANP-HRP) are pipetted into the wells of the microtiter strips, which are pre-coated with polyclonal sheep anti-NT-proANP antibody. NT-proANP present in the sample binds to the pre-coated antibody in the well and forms a sandwich with the conjugate. In the washing step all non-specific unbound material is removed. In a second step, the substrate (TMB Tetramethylbenzidine) is pipetted into the wells. The enzyme catalyzed color change of the substrate is directly proportional to the amount of NT-proANP present in the sample. This color change is detectable with a standard microtiter plate ELISA reader.
The NT-proANP ELISA kit uses highly purified, epitope-mapped antibodies. The antibodies utilized in the NT-proANP ELISA (BI-20892) are as follows:
Capture antibody: AA 1-30 (polyclonal sheep anti-human NT-proANP 1-98)
Detection antibody: AA 79-98 (HRP-labeled polyclonal sheep anti-human NT-proANP 1-98)
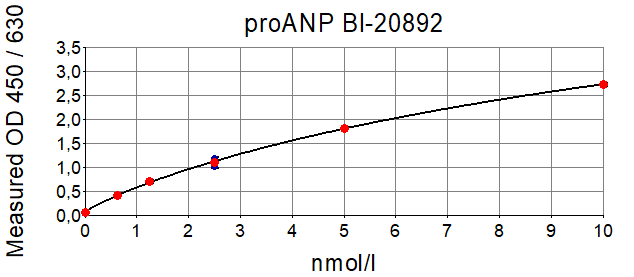
Typical Standard Curve
The figure below shows a typical standard curve for the NT-proANP (or proANP (1-98)) ELISA. The immunoassay is calibrated against human recombinant NT-proANP (or proANP (1-98)) peptide:
ELISA Kit Components
|
Contents |
Description |
Quantity |
|
PLATE |
Polyclonal sheep anti-human NT-proANP antibody pre-coated microtiter strips in a strip holder, packed in an aluminum bag with desiccant |
12 x 8 tests |
|
WASHBUF |
Wash buffer concentrate 20x, natural cap |
1 x 50 ml |
|
STD |
Standards 1-6, (0; 0.63; 1.25; 2.5; 5; 10 nmol/l), synthetic human NT-proANP in human plasma, white caps, lyophilized |
6 vials |
|
CTRL |
Control, yellow cap, lyophilized, exact concentration see label |
1 vial |
|
ASYBUF |
Assay buffer, red cap, ready to use |
1 x 25 ml |
|
CONJ |
Conjugate (polyclonal sheep anti-human NT-proANP-HRP), amber cap, ready to use |
1 x 22 ml |
|
SUB |
Substrate (TMB solution), amber bottle, blue cap, ready to use |
1 x 22 ml |
|
STOP |
Stop solution, white cap, ready to use |
1 x 7 ml |
Serum, EDTA plasma, heparin plasma, citrate plasma, cell culture supernatant and urine are suitable for use in this assay. Do not change sample type during studies. We recommend duplicate measurements for all samples, standards and controls. The sample collection and storage conditions listed are intended as general guidelines.
Serum & Plasma
Collect venous blood samples in standardized serum separator tubes (SST) or standardized blood collection tubes using EDTA, heparin or citrate as an anticoagulant. Serum separation should be performed within one hour after blood collection. For serum samples, allow samples to clot for 30 minutes at room temperature. Perform separation by centrifugation according to the tube manufacturer’s instructions for use. Assay the acquired samples immediately or aliquot and store at -25°C or lower. Lipemic or haemolyzed samples may give erroneous results.
Serum samples should not be subjected to more than two freeze-thaw cycles. EDTA plasma samples can undergo three freeze-thaw cycles.
Urine
Note: the experiments performed to measure NT-proANP in urine samples has not undergone a full validation according to ICH guidelines. However, our performance check suggests that urine samples can be measured with this ELISA. For more information please refer to our validation data.
Aseptically collect the first urine of the day (mid-stream), voided directly into a sterile container. Centrifuge to remove particulate matter, assay immediately or aliquot and store at -25°C or lower.
Cell Culture Supernatant
Note: the experiments performed to measure NT-proANP in cell culture supernatant samples has not undergone a full validation according to ICH guidelines. However, our performance check suggests that cell culture supernatant samples can be measured with this ELISA. For more information please refer to our validation data.
Remove particulates by centrifugation and assay immediately or aliquot and store samples at
-25°C or lower. Do not freeze-thaw samples more than three times.
Reagent Preparation
Wash Buffer
|
1. |
Bring the WASHBUF concentrate to room temperature. Crystals in the buffer concentrate will dissolve at room temperature (18-26°C). |
|
2. |
Dilute the WASHBUF concentrate 1:20, e.g. 50 ml WASHBUF + 950 ml distilled or deionized water. Only use diluted WASHBUF when performing the assay. |
The diluted WASHBUF is stable up to one month at 4°C (2-8°C).
Standards & Controls for Serum, Plasma and Urine Measurements
|
1. |
Pipette 250 µl of distilled or deionized water into each standard (STD) and control (CTRL) vial. The exact concentration is printed on the label of each vial. |
|
2. |
Leave at room temperature (18-26°C) for 15 min. Vortex gently. |
Reconstituted STDs and CTRL are stable at -25°C or lower until expiry date stated on the label. Avoid freeze-thaw cycles!
Standards for Cell Culture Supernatant Measurements
For the preparation of cell culture-based standards always use the identical cell culture medium (CCM) as used for the experiment.
|
1. |
Reconstitute standard 7 (STD7) in 200 µl deionized water. Leave at room temperature (18-26°C) for 15 min and mix well before making dilutions. Use polypropylene tubes. |
|
2. |
Mark tubes ccSTD6 to ccSTD1. Dispense 100 µl cell culture medium into each vial. |
|
3. |
Pipette 100 µl of STD7 into tube marked as ccSTD6. Mix thoroughly. |
|
4. |
Transfer 100 µl of ccSTD6 into the tube marked as ccSTD5. Mix thoroughly. |
|
5. |
Continue in the same fashion to obtain ccSTD4 to ccSTD2. CCM serves as the ccSTD1 (0 nmol/l NT-proANP). |
|
6. |
Using the prepared standards, follow the protocol as indicated for serum and plasma samples. |
Attention: Supplied STD1-STD7 and controls are only valid for serum or plasma and should not be used for cell culture measurements.
Sample Preparation
Bring samples to room temperature and mix samples gently to ensure the samples are homogenous. We recommend duplicate measurements for all samples. Samples for which the optical density (OD) value exceeds the highest point of the standard range (STD6, 10 nmol/l) can be diluted with ASYBUF (Assay buffer).
Assay Protocol
Read the entire protocol before beginning the assay.
|
1. |
Bring samples and reagents to room temperature (18-26°C). |
|
2. |
Mark positions for STD/SAMPLE/CTRL (Standard/Sample/Control) on the protocol sheet. |
|
3. |
Take microtiter strips out of the aluminum bag. Store unused strips with desiccant at 4°C in the aluminum bag. Strips are stable until expiry date stated on the label. |
|
4. |
Pipette 10 µl STD/CTRL/SAMPLE in duplicates into the respective wells. |
|
5. |
Add 200 µl CONJ (Conjugate, amber cap) into each well, swirl gently. |
|
6. |
Cover the plate tightly, swirl gently and incubate for 3 hours at room temperature (18-24°C) in the dark. |
|
7. |
Aspirate and wash wells 5x with 300 µl diluted WASHBUF. After the final wash, remove the remaining WASHBUF by strongly tapping plate against a paper towel. |
|
8. |
Add 200 µl SUB (substrate, blue cap) into each well, swirl gently. |
|
9. |
Incubate for 30 min at room temperature (18-24°C) in the dark. |
|
10. |
Add 50 µl STOP (stop solution, white cap) into each well, swirl gently. |
|
11. |
Measure absorbance immediately at 450 nm with reference 630 nm, if available. |
Calculation of Results
Read the optical density (OD) of all wells on a plate reader using 450 nm wavelength (reference wavelength 630 nm). Construct a standard curve from the absorbance read-outs of the standards using commercially available software capable of generating a four-parameter logistic (4-PL) fit. Alternatively, plot the standards’ concentration on the x-axis against the mean absorbance for each standard on the y-axis and draw a best fit curve through the points on the graph. Curve fitting algorithms other than 4-PL have not been validated and will need to be evaluated by the user.
Obtain sample concentrations from the standard curve. If required, nmol/l can be converted into ng/ml by applying a conversion factor (1 nmol/l = 12.7 ng/ml or 1 ng/ml = 0.079 nmol/l (MW: 12.7 kDa)). Respective dilution factors must be considered when calculating the final concentration of the sample.
The quality control protocol supplied with the kit shows the results of the final release QC for each kit. ODs obtained by customers may differ due to various influences including a normal decrease of signal intensity throughout shelf life. However, this does not affect validity of results as long as an OD of 1.00 or higher is obtained for STD 6 and the value of the CTRL is within the target range (see label).
INFORMATION ON THE ANALYTE
NT-proANP Protein
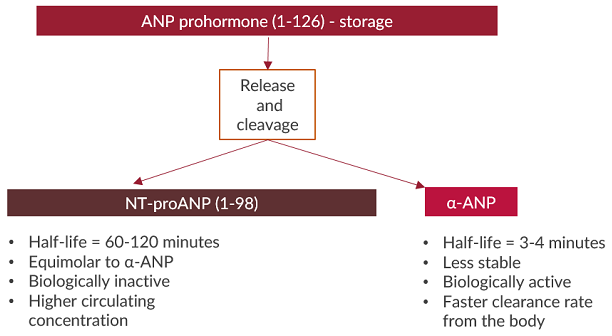
N-terminal proatrial natriuretic peptide (NT-proANP 1-98) is the biologically inactive fragment (98 amino acid) of the ANP prohormone.
ANP is translated from its gene as a 151-amino acid precursor, pre-proANP. After removal of the 25-amino acid signal peptide, the tissue form of the hormone, a 126-amino acid proANP (γ-ANP) is generated. γ-ANP is proteolytically cleaved to the biologically active ANP (α-ANP) and to the 98 amino acid NT-proANP peptide (also known as proANP 1-98). The major molecular forms of circulating human ANP is thus the 28 amino-acid peptide (α-ANP) that contains a ring structure with a disulfide bridge and the 98-amino acid NT-proANP peptide, which is easier to detect in the circulation due to its longer half-life. Both peptides α-ANP and NT-proANP circulate in equimolar amounts.
ANP is secreted from the heart in response to atrial stretching or through stimulation by angiotensin II and endothelin. The most important stimulus for the release of the hormone into circulation is stretching of myocyte fibres. On release, the prohormone is split into equimolar amounts of the highly biologically active proANP (99-126), also known as -ANP or ANP, and the N-terminal part proANP (1-98) (also known as NT-proANP) (Nakagawa et al., 2019; Volpe et al., 2015).
NT-proANP is more stable and has a longer half-life (60-120 min) in circulation than ANP which is rapidly cleared from the circulation with a half-life of 3-4 minutes (Yandle et al., 1986). The natriuretic peptides have a common characteristic biochemical structure that consists of a ring of 17 amino acids and a disulfide bridge between 2 cysteine molecules (Clerico et al., 2011; Volpe et al., 2015; Yandle et al., 1986).
The ANP prohormone undergoes several cleavages to generate the biologically active form of the hormone. N-terminal (NT) prohormone fragments of natriuretic peptides are typically more stable, have longer half-lives, and circulate at higher concentrations compared to C-terminal biologically active hormone ends (Yandle et al., 1986). It has therefore been suggested that measuring NT prohormone fragments of ANP provide more accurate concentrations in samples (Clerico et al., 2011).
The expression and secretion of ANP increase significantly in pathological states accompanied by stretching the heart chambers, volume overload, and ischemic injury, such as heart failure and myocardial infarction.
|
Molecular Weight |
12.7 kDa |
|
Cellular localisation |
ANP is primarily expressed and stored in granules in the atria; secreted |
|
Post-translational modifications |
Not known |
|
Sequence similarities |
Natriuretic peptide family |
|
Alternative Names |
Official name: natriuretic peptide A ANF; ANP; CDD; CDP; PND; ATFB6; ATRST2; CDD-ANF |
|
Entrez/NCBI ID |
Gene ID: 4878 |
|
Genecards |
NPPA: https://www.genecards.org/cgi-bin/carddisp.pl?gene=NPPA&keywords=nppa |
|
OMIM |
|
|
PDB |
|
|
Pfam |
|
|
Protein Atlas |
NPPA: https://www.proteinatlas.org/ENSG00000175206-NPPA/tissue |
|
Uniport ID |
NT-proANP Function
The natriuretic peptide NT-proANP and the biologically active ANP are synthesized from the cardiac myocytes, after proteolytical cleavage from the proANP prohormone. The primary stimulus for ANP release is atrial wall stretch resulting from increased intravascular volume. Once secreted, ANP perfuses into the coronary sinus, which facilitates distribution to its various target organs in an endocrine manner. Hormones such as endothelin, angiotensin and arginine–vasopressin stimulate ANP release (Volpe et al., 2015).
Bioactive ANP regulates blood pressure by promoting sodium and water excretion. ANP causes a reduction in expanded extracellular fluid volume by increasing renal sodium excretion. The cardiac muscle cells of the heart contain volume receptors which respond to increased stretching of the atrial wall due to increased atrial blood volume. In addition, ANP shows endocrine and metabolic effects which includes the inhibition of aldosterone and vasopressin. ANP also plays a role in other endocrine functions such as cortisol secretion and it enhances lipolysis and the release of testosterone and insulin (Clerico et al., 2011; Volpe et al., 2015). ANP also plays an immunregulatory role as it is upregulated in activated macrophages promoting microbial clearance (Volpe et al., 2015).
NT-proANP has been shown to be a useful diagnostic and prognostic tool in heart failure and myocardial infarction. In patients with mild to moderate cardiac disease, NT-proANP levels were increased in response to atrial wall stress increase. Patients diagnosed with diastolic or systolic dysfunction had 2- to 3-fold higher NT-proANP than the control group (Berger et al., 2005; Volpe et al., 2015).
Hulsmann and coworkers could demonstrate that NT-proANP appears to be a more sensitive marker than BNP or NT-proBNP with respect to the impact on survival in patients with
chronic heart failure (Hülsmann et al., 2005). A study by Squire and co-workers showed that in patients following acute myocardial infarction NT-proBNP predicts 30-day and NT-proANP later than 30-day mortality (Squire et al., 2004). From this study the authors conclude that consideration of both, NT-proANP and NT-proBNP, identifies a greater number of patients at risk of death or heart failure than either peptide alone (Squire et al., 2004).
Several studies successfully demonstrated that this NT-proANP ELISA is suitable for rat and cat samples and can be used in preclinical toxicology investigations (Colton et al., 2011; Dunn et al., 2017; Kim et al., 2016; Parzeniecka-Jaworska et al., 2016; Turner et al., 2018; Vinken et al., 2016; Zimmering et al., 2010). Vinken and colleagues demonstrated in a cross-laboratory analytical validation that this assay is technically adequate for the detection of NT-proANP serum levels in SD rats (Vinken et al., 2016). Numerous investigations have shown that NT-proANP is an excellent cardiovascular safety biomarker in rats (Dunn et al., 2017; Kim et al., 2016; Vinken et al., 2016).
-
Heart Disease
Chronic heart failure (Hülsmann et al., 2005)
Heart failure (Eriksson et al., 2014; Luers et al. 2013)
Risk assessment in heart failure patients (Berger et al., 2005)
Risk assessment in myocardial infarction patients with normal NT-proBNP levels (Squire et al., 2004)
NT-proANP as marker of response to resynchronisation therapy (Molhoek et al., 2004)
-
Infectious Disease
Sepsis (Hoffmann et al., 2005)
-
Kidney Disease
ANP plays physiological roles in the renal system such as increasing renal blood flow and glomerular filtration rate (GFR). (Volpe et al., 2015)
-
Metabolic Disease
Diabetes and obesity: Evidence suggests that ANP can influence glucose and fat metabolism by increasing adiponectin levels and can protect against the onset of diabetes. These findings suggest that ANP levels can help to further understand the connection between diabetes and cardiovascular disease. (Birkenfeld et al., 2012; Gurden et al., 2014; Jujic et al., 2014)
Literature
Atrial and brain natriuretic peptides: Hormones secreted from the heart.
Nakagawa, Y., Nishikimi, T., Kuwahara, K., 2019. Peptides 111, 18–25. PMID: 29859763
PMID: 29859763
FGF21 increases water intake, urine output and blood pressure in rats.
Turner, T., Chen, X., Zahner, M., Opsahl, A., DeMarco, G., Boucher, M., Goodwin, B., Perreault, M., 2018. PLOS ONE 13, e0202182.PMID: 30106981
Serum Natriuretic Peptides as Differential Biomarkers Allowing for the Distinction between Physiologic and Pathologic Left Ventricular Hypertrophy.
Dunn, M.E., Manfredi, T.G., Agostinucci, K., Engle, S.K., Powe, J., King, N.M.P., Rodriguez, L.A., Gropp, K.E., Gallacher, M., Vetter, F.J., More, V., Shimpi, P., Serra, D., Colton, H.M., Cardiac Hypertrophy Working Group of the Predictive Safety Testing Consortium, 2017. Toxicol Pathol 45, 344–352.PMID: 27102652
Evaluation of Cardiac Toxicity Biomarkers in Rats from Different Laboratories.
Kim, K., Chini, N., Fairchild, D.G., Engle, S.K., Reagan, W.J., Summers, S.D., Mirsalis, J.C., 2016. Toxicol Pathol 44, 1072–1083.PMID: 27638646; PMCID: PMC5330931
ProANP as a screening biomarker for hypertrophic cardiomyopathy in Maine coon cats.
Parzeniecka-Jaworska, M., Garncarz, M., Kluciński, W., 2016. Polish Journal of Veterinary Sciences 19, 801–807.PMID: 28092607
Cross-laboratory analytical validation of the cardiac biomarker NT-proANP in rat.
Vinken, P., Reagan, W.J., Rodriguez, L.A., Buck, W.R., Lai-Zhang, J., Goeminne, N., Barbacci, G., Liu, R., King, N.M.P., Engle, S.K., Colton, H., 2016. Journal of Pharmacological and Toxicological Methods 77, 58–65.PMID: 26516096
The natriuretic peptides system in the pathophysiology of heart failure: from molecular basis to treatment.
Volpe, M., Carnovali, M., Mastromarino, V., 2015. Clinical Science 130, 57–77.PMID: 26637405
Increased NT-proANP predicts risk of congestive heart failure in Cavalier King Charles spaniels with mitral regurgitation caused by myxomatous valve disease.
Eriksson, A.S., Häggström, J., Pedersen, H.D., Hansson, K., Järvinen, A.-K., Haukka, J., Kvart, C., 2014. J Vet Cardiol 16, 141–154.PMID: 25130405
Natriuretic peptides, heart, and adipose tissue: new findings and future developments for diabetes research.
Gruden, G., Landi, A., Bruno, G., 2014. Diabetes Care 37, 2899–2908.PMID: 25342830
Atrial natriuretic peptide and type 2 diabetes development--biomarker and genotype association study. Jujić, A., Nilsson, P.M., Engström, G., Hedblad, B., Melander, O., Magnusson, M., 2014. PLoS ONE 9, e89201.
PMID: 24586593; PMCID: PMC3929630
NT-proANP and NT-proBNP as prognostic markers in patients with acute decompensated heart failure of different etiologies.
Luers, C., Sutcliffe, A., Binder, L., Irle, S., Pieske, B., 2013. Clinical Biochemistry 46, 1013–1019.PMID: 23542086
Atrial natriuretic peptide and adiponectin interactions in man.
Birkenfeld, A.L., Boschmann, M., Engeli, S., Moro, C., Arafat, A.M., Luft, F.C., Jordan, J., 2012. PLoS ONE 7, e43238.PMID: 22916229; PMCID: PMC3420865
Thirty years of the heart as an endocrine organ: physiological role and clinical utility of cardiac natriuretic hormones.
Clerico, A., Giannoni, A., Vittorini, S., Passino, C., 2011. Am. J. Physiol. Heart Circ. Physiol. 301, H12-20.PMID: 21551272
An initial characterization of N-terminal-proatrial natriuretic peptide in serum of Sprague Dawley rats.
Colton, H.M., Stokes, A.H., Yoon, L.W., Quaile, M.P., Novak, P.J., Falls, J.G., Kimbrough, C.L., Cariello, N.F., Jordan, H.L., Berridge, B.R., 2011. Toxicol. Sci. 120, 262–268.PMID: 21242511
Evaluation of the association between plasma concentration of N-terminal proatrial natriuretic peptide and outcome in cats with cardiomyopathy.
Zimmering, T.M., Hungerbühler, S., Meneses, F., Nolte, I., Simon, D., 2010. Journal of the American Veterinary Medical Association 237, 665–672.PMID: 20839988
Neurohormonal risk stratification for sudden death and death owing to progressive heart failure in chronic heart failure.
Berger, R., Huelsmann, M., Strecker, K., Moertl, D., Moser, P., Bojic, A., Pacher, R., 2005. Eur. J. Clin. Invest. 35, 24–31.PMID: 15638816
Increased plasma levels of NT-proANP and NT-proBNP as markers of cardiac dysfunction in septic patients.
Hoffmann, U., Brueckmann, M., Bertsch, T., Wiessner, M., Liebetrau, C., Lang, S., Haase, K.K., Borggrefe, M., Huhle, G., 2005. Clin. Lab. 51, 373–379.PMID: 16122147
Incidence of normal values of natriuretic peptides in patients with chronic heart failure and impact on survival: a direct comparison of N-terminal atrial natriuretic peptide, N-terminal brain natriuretic peptide and brain natriuretic peptide.
Hülsmann, M., Berger, R., Mörtl, D., Gore, O., Meyer, B., Pacher, R., 2005. Eur. J. Heart Fail. 7, 552–556.PMID: 15921794
Atrial and brain natriuretic peptides as markers of response to resynchronisation therapy.
Molhoek, S.G., Bax, J.J., van Erven, L., Bootsma, M., Steendijk, P., Lentjes, E., Boersma, E., van der Laarse, A., van der Wall, E.E., Schalij, M.J., 2004. Heart 90, 97–98.PMID: 14676258; PMCID: PMC1768004
N-terminal pro-atrial natriuretic peptide (N-ANP) and N-terminal pro-B-type natriuretic peptide (N-BNP) in the prediction of death and heart failure in unselected patients following acute myocardial infarction.
Squire, I.B., O’Brien, R.J., Demme, B., Davies, J.E., Ng, L.L., 2004. Clin. Sci. 107, 309–316.PMID: 15182235
Metabolic clearance rate and plasma half life of alpha-human atrial natriuretic peptide in man.
Yandle, T.G., Richards, A.M., Nicholls, M.G., Cuneo, R., Espiner, E.A., Livesey, J.H., 1986. Life Sci. 38, 1827–1833.PMID: 2939312
All Biomedica ELISAs are validated according to international FDA/ICH/EMEA guidelines. For more information about our validation guidelines, please refer to our quality page and published validation guidelines and literature.
1. ICH Q2(R1) Validation of Analytical Procedures: Text and Methodology.
2. EMEA/CHMP/EWP/192217/2009 Guideline on bioanalytical method validation.
3. Bioanalytical Method Validation, Guidance for Industry, FDA, May 2018
Calibration
This immunoassay is calibrated against recombinant NT-proANP. Analysis of the recombinant standard material has been performed by SDS-PAGE electrophoresis and MALDI-TOF MS spectrum.
Sequence: MKYTAWPHNPMYNAVSNADLMDFKNLLDHLEEKMPLEDEVVPPQVLSEPNEEAGAALSPL PEVPPWTGEVSPAQRDGGALGRGPWDSSDRSALLKSKLRALLTAPRLEHHHHHH
Molecular Weight: 12.7 kDa
Detection Limit & Sensitivity
To determine the sensitivity of the NT-proANP ELISA, experiments measuring the lower limit of detection (LOD) and the lower limit of quantification (LLOQ) were conducted.
The LOD, also called the detection limit, is the lowest point at which a signal can be distinguished above the background signal, i.e. the signal that is measured in the absence of NT-proANP, with a confidence level of 99%. It is defined as the mean back calculated concentration of standard 1 (0 pmol/l of NT-proANP, five independent measurements) plus three times the standard deviation of the measurements.
The LLOQ, or sensitivity of an assay, is the lowest concentration at which an analyte can be accurately quantified. The criteria for accurate quantification at the LLOQ are an analyte recovery between 75 and 125% and a coefficient of variation (CV) of less than 25%. To determine the LLOQ, standard 2, i.e. the lowest standard containing NT-proANP, is diluted, measured five times and its concentration back calculated. The lowest dilution, which meets both criteria, is reported as the LLOQ.
The following value was determined for the NT-proANP ELISA:
|
LOD |
0.05 nmol/l |
|
LLOQ |
0.08 nmol/l |
Precision
The precision of an ELISA is defined as its ability to measure the same concentration consistently within the same experiments carried out by one operator (within-run precision or repeatability) and across several experiments using the same samples but conducted by several operators using different ELISA lots (in-between-run precision or reproducibility).
Within-Run Precision
Within-run (intra-assay) precision was assessed by measuring two samples of known concentrations five times within one NT-proANP ELISA kit lot by one operator.
|
ID |
Within-Run Precision n |
Mean NT-proANP [pmol/l] |
SD [pmol/l] |
CV (%) |
|
Sample 1 |
5 |
1.07 |
0.05 |
5 |
|
Sample 2 |
5 |
7.58 |
0.16 |
2 |
In-Between-Run Precision
In-between-run (intra-assay) precision was assessed by measuring two samples three times within three different NT-proANP ELISA kit lots by two different operators.
|
ID |
In-Between Run Precision n |
Mean NT-proANP [pmol/l] |
SD [pmol/l] |
CV [%] |
|
Sample 1 |
3 |
1.11 |
0.10 |
9 |
|
Sample 2 |
3 |
7.24 |
0.37 |
5 |
Accuracy
The accuracy of an ELISA is defined as the precision with which it can recover samples of known concentrations.
The recovery of the NT-proANP ELISA was measured by adding recombinant NT-proANP to human samples containing a known concentration of endogenous NT-proANP. The % recovery of the spiked concentration was calculated as the percentage of measured compared over the expected value.
This table shows the summary of the recovery experiments in the NT-proANP ELISA in EDTA plasma samples:
|
|
% Recovery |
||||
|
Sample Matrix |
n |
+0.81 nmol/l |
+4.05 nmol/l |
||
|
Mean |
Range |
Mean |
Range |
||
|
EDTA plasma |
4 |
87 |
82-90 |
89 |
84-98 |
Data showing recovery of recombinant NT-proANP in human EDTA plasma samples:
|
NT-proANP [nmol/l] |
% Recovery |
|||||
|
Sample Matrix |
ID |
Reference |
+0.81 nmol/l |
+4.05 nmol/l |
+0.81 nmol/l |
+4.05 nmol/l |
|
EDTA-plasma |
e1 |
1,53 |
1,96 |
4,70 |
84% |
84% |
|
EDTA-plasma |
e2 |
0,53 |
1,10 |
3,99 |
82% |
87% |
|
EDTA-plasma |
e3 |
0,80 |
1,47 |
4,75 |
91% |
98% |
|
EDTA-plasma |
e4 |
0,87 |
1,51 |
4,20 |
90% |
85% |
|
Mean |
87 |
89 |
||||
|
Min |
82 |
84 |
||||
|
Max |
91 |
98 |
||||
Dilution Linearity
Tests of dilution linearity ensure that samples containing recombinant NT-proANP behave in a dose dependent manner and are not affected by matrix effects. Dilution linearity assesses the accuracy of measurements in diluted clinical samples spiked with known concentrations of recombinant analyte. Dilution linearity was assessed for each sample type and was considered acceptable if the results are within ± 20% of the expected concentration.
Dilution linearity was assessed by serially diluting human samples spiked with human recombinant NT-proANP with assay buffer.
The table below show the mean recovery of serially diluted recombinant NT-proANP in human EDTA plasma samples:
|
Sample Matrix |
n |
1+1 |
1+4 |
1+9 |
|||
|
Mean |
Range |
Mean |
Range |
Mean |
Range |
||
|
EDTA plasma |
3 |
90 |
88-92 |
91 |
78-115 |
79 |
73-92 |
Data showing dilution linearity of 4.0 nmol/l recombinant NT-proANP spiked into human EDTA plasma samples:
|
NT-proANP [nmol/l] |
% Recovery |
||||||||
|
Sample Matrix |
ID |
Reference |
1+1 |
1+4 |
1+9 |
1+1 |
1+4 |
1+9 |
|
|
EDTA plasma |
e1 |
4.42 |
1.97 |
1.02 |
0.32 |
89 |
115 |
73 |
|
|
EDTA plasma |
e2 |
3.68 |
11.02 |
0.58 |
0.34 |
92 |
78 |
92 |
|
|
EDTA plasma |
e3 |
3.75 |
1.97 |
0.61 |
0.34 |
88 |
81 |
X |
|
|
|
Mean |
90 |
91 |
79 |
|||||
|
|
Min |
88 |
78 |
73 |
|||||
|
|
Max |
92 |
115 |
92 |
|||||
Specificity
This assay recognizes endogenous (natural) and recombinant NT-proANP.
Cross Reactivity
Cross reactivity was tested on a panel of related molecules.
proANP (1-30) <1%, proANP (31-67) <1%, proANP (79-98) <1%, alpha ANP (99-126) <1%, proBNP (8-29) <1%, proBNP (32-57) <1%, proCNP (1-19) <1%, proCNP (30-50) <1%, proCNP (51-97) <1%.
This assay is also suitable for the detection of rat and mouse NT-proANP as well as cat NT-proANP as shown in various preclinical studies.
NT-proANP Values in Mouse Samples
The graph below shows NT-proANP data from a study using mouse samples.
Mouse samples were assayed with this NT-proANP ELISA. The results indicate that mouse samples can be measured with this ELISA.

NT-proANP Values in Rat Samples
References for NT-proANP ELISA in RAT samples:
An initial characterization of N-terminal-proatrial natriuretic peptide in serum of Sprague Dawley rats.
Colton, H.M., Stokes, A.H., Yoon, L.W., Quaile, M.P., Novak, P.J., Falls, J.G., Kimbrough, C.L., Cariello, N.F., Jordan, H.L., Berridge, B.R., 2011. Toxicol. Sci. 120, 262–268.
PMID: 21242511
Cross-laboratory analytical validation of the cardiac biomarker NT-proANP in rat.
Vinken, P., Reagan, W.J., Rodriguez, L.A., Buck, W.R., Lai-Zhang, J., Goeminne, N., Barbacci, G., Liu, R., King, N.M.P., Engle, S.K., Colton, H., 2016. Journal of Pharmacological and Toxicological Methods 77, 58–65.
Serum Natriuretic Peptides as Differential Biomarkers Allowing for the Distinction between Physiologic and Pathologic Left Ventricular Hypertrophy.
Dunn, M.E., Manfredi, T.G., Agostinucci, K., Engle, S.K., Powe, J., King, N.M.P., Rodriguez, L.A., Gropp, K.E., Gallacher, M., Vetter, F.J., More, V., Shimpi, P., Serra, D., Colton, H.M., Cardiac Hypertrophy Working Group of the Predictive Safety Testing Consortium, 2017. Toxicol Pathol 45, 344–352.
PMID: 27102652
FGF21 increases water intake, urine output and blood pressure in rats.
Turner, T., Chen, X., Zahner, M., Opsahl, A., DeMarco, G., Boucher, M., Goodwin, B., Perreault, M., 2018. PLOS ONE 13, e0202182.
Evaluation of Cardiac Toxicity Biomarkers in Rats from Different Laboratories.
Kim, K., Chini, N., Fairchild, D.G., Engle, S.K., Reagan, W.J., Summers, S.D., Mirsalis, J.C., 2016. Toxicol Pathol 44, 1072–1083.
PMID: 27638646; PMCID: PMC5330931
NT-proANP Values in Cat Samples
References for NT-proANP ELISA in Cat samples:
Evaluation of the association between plasma concentration of N-terminal proatrial natriuretic peptide and outcome in cats with cardiomyopathy.
Zimmering, T.M., Hungerbühler, S., Meneses, F., Nolte, I., Simon, D., 2010. Journal of the American Veterinary Medical Association 237, 665–672.
ProANP as a screening biomarker for hypertrophic cardiomyopathy in Maine coon cats.
Parzeniecka-Jaworska, M., Garncarz, M., Kluciński, W., 2016. Polish Journal of Veterinary Sciences 19, 801–807.
Sample Stability
The stability of endogenous NT-proANP was tested by comparing NT-proANP measurements in samples that had undergone three freeze-thaw cycles.
For freeze-thaw experiments, samples were collected according to the supplier’s instruction using blood collection devices and stored at -80°C. Reference samples were freeze-thawed once. The mean recovery of sample concentration after three freeze-thaw cycles is 85%.
|
|
NT-proANP [nmol/l] |
% Recovery 3 F/T vs ref |
|||
|
Sample ID EDTA-plasma |
Reference |
1x |
2x |
3x |
|
|
#E1 |
1.02 |
0.96 |
0.82 |
1.02 |
80% |
|
#E2 |
5.44 |
5.42 |
4.75 |
5.44 |
87% |
|
#E3 |
0.66 |
0.61 |
0.59 |
0.66 |
90% |
|
#E4 |
1.54 |
1.52 |
1.23 |
1.54 |
80% |
|
#E5 |
3.97 |
3.46 |
3.42 |
3.97 |
86% |
|
Mean |
85% |
||||
Samples can undergo at least up to three freeze-thaw cycles.
Short-Term Stability
Freshly collected matched pairs of serum and plasma samples (n=13) were kept at room temperature (18-26°C) for different time periods. Aliquots were drawn and immediately frozen at -70°C and assayed all together the next day in one test run. The graph below summarizes the data obtained:
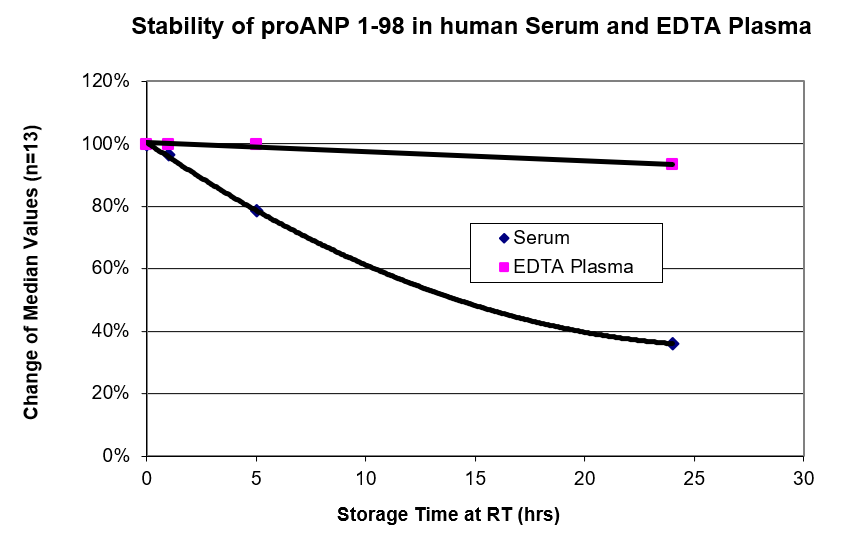
NT-proANP is not stable in serum samples for a longer storage time at room temperature. Therefore, serum separation should be performed within one hour after blood collection. Allow serum samples to clot for 30 minutes at room temperature. Perform separation by centrifugation according to the tube manufacturer’s instructions for use. Assay the acquired samples immediately or aliquot and store at -25°C or lower. Serum samples should not be subjected to more than two freeze-thaw cycles.
Sample Values
NT-proANP Values in Apparently Healthy Donors
NT-proANP reference ranges were established from EDTA plasma samples from apparently healthy donors (age 20-64 years). No medical histories were available for the volunteers.
|
Sample Matrix |
n |
Median [nmol/l] |
Range [nmol/l] |
|
EDTA plasma |
53 |
1.45 |
0.8 – 2.5 |
It is recommended to establish the normal range for each laboratory.
NT-proANP Values in an Unselected Hospital Panel
NT-proANP was measured in patients from an unselected hospital panel. No medical histories were available.
|
Sample Matrix |
EDTA-plasma |
|
n |
40 |
|
Mean [nmol/l] |
3.89 |
|
Median [nmol/l] |
3.09 |
|
Min [nmol/l] |
0.63 |
|
Max [nmol/l] |
10.50 |
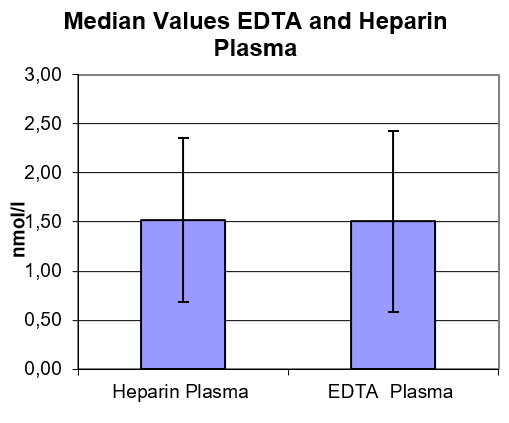
Matrix Comparision
To assess whether all different plasma matrices behave the same way in the NT-proANP ELISA, concentrations of NT-proANP were measured in EDTA and heparin plasma. Samples were prepared from 13 apparently healthy donors. Each individual donated blood in all tested sample matrices. Heparin and EDTA plasma show nearly identical NT-proANP values.
-
Acute effects of insulin on circulating natriuretic peptide levels in humans.
Bachmann, K.N., Deger, S.M., Alsouqi, A., Huang, S., Xu, M., Ferguson, J.F., Su, Y.R., Niswender, K.D., Ikizler, T.A., Wang, T.J., 2018. PLOS ONE 13, e0196869.
-
Castagna, O., Regnard, J., Gempp, E., Louge, P., Brocq, F.X., Schmid, B., Desruelle, A.-V., Crunel, V., Maurin, A., Chopard, R., MacIver, D.H., 2018. Sports Medicine - Open 4, 1.
-
Role of the Lymphatic System in the Pathogenesis of Hypertension in Humans.
Chachaj, A., Puła, B., Chabowski, M., Grzegrzółka, J., Szahidewicz-Krupska, E., Karczewski, M., Janczak, D., Dzięgiel, P., Podhorska-Okołów, M., Mazur, G., Gamian, A., Szuba, A., 2018. Lymphat Res Biol 16, 140–146.
PMID: 29346014 -
Plasma levels of heart failure biomarkers are primarily a reflection of extracardiac production.
Du, W., Piek, A., Schouten, E.M., van de Kolk, C.W.A., Mueller, C., Mebazaa, A., Voors, A.A., de Boer, R.A., Silljé, H.H.W., 2018. Theranostics 8, 4155–4169.
PMID: 30128044; PMCID: PMC6096401 -
FGF21 increases water intake, urine output and blood pressure in rats.
Turner, T., Chen, X., Zahner, M., Opsahl, A., DeMarco, G., Boucher, M., Goodwin, B., Perreault, M., 2018. PLOS ONE 13, e0202182.
-
Association of NT-proANP Level in Plasma and Humor Aqueous with Primary Open-Angle Glaucoma.
Baumane, K., Ranka, R., Laganovska, G., 2017. Current Eye Research 42, 233–236.
PMID: 27723368 -
Dunn, M.E., Manfredi, T.G., Agostinucci, K., Engle, S.K., Powe, J., King, N.M.P., Rodriguez, L.A., Gropp, K.E., Gallacher, M., Vetter, F.J., More, V., Shimpi, P., Serra, D., Colton, H.M., Cardiac Hypertrophy Working Group of the Predictive Safety Testing Consortium, 2017. Toxicol Pathol 45, 344–352.
PMID: 27102652 -
Li, V.W., Lai, C.T., Liu, A.P., Cheuk, D.K., Cheung, Y., 2017. Ultrasound in Medicine & Biology 43, 1897–1905.
-
Prysyazhnyuk, V.P., Voloshyn, O.I., 2017. The Pharma Innovation Journal 6, 386–389
-
Straub, R.H., Ehrenstein, B., Günther, F., Rauch, L., Trendafilova, N., Boschiero, D., Grifka, J., Fleck, M., 2017. Clin. Rheumatol. 36, 1041–1051.
PMID: 27112146 -
Wakula, P., Neumann, B., Kienemund, J., Thon-Gutschi, E., Stojakovic, T., Manninger, M., Scherr, D., Scharnagl, H., Kapl, M., Pieske, B., Heinzel, F.R., 2017. Europace 19, 544–551.
PMID: 28431065 -
Identification and functional analysis of CORIN variants in hypertensive patients.
Zhang, Yue, Zhou, T., Niu, Y., He, M., Wang, C., Liu, M., Yang, J., Zhang, Yonghong, Zhou, J., Fukuda, K., Qin, J., Dong, N., Wu, Q., 2017. Human Mutation 38, 1700–1710.
-
Association between plasma proANP and hyperuricemia in Chinese Han women: a cross-sectional study.
Zhu, Z., Zhang, Q., Peng, H., Zhong, C., Liu, Y., Huangfu, X., Tian, Y., Chao, X., Jin, J., Zhang, Y., 2017a. Clinical Chemistry and Laboratory Medicine (CCLM) 55, 1160–1167.
-
Zhu, Z., Zhang, Q., Peng, H., Zhong, C., Liu, Y., Huangfu, X., Tian, Y., Chao, X., Wang, A., Jin, J., Zhang, Y., 2017b. Clinica Chimica Acta 469, 26–30.
-
Hughson, R.L., Robertson, A.D., Arbeille, P., Shoemaker, J.K., Rush, J.W.E., Fraser, K.S., Greaves, D.K., 2016. American Journal of Physiology-Heart and Circulatory Physiology 310, H628–H638.
-
Evaluation of Cardiac Toxicity Biomarkers in Rats from Different Laboratories.
Kim, K., Chini, N., Fairchild, D.G., Engle, S.K., Reagan, W.J., Summers, S.D., Mirsalis, J.C., 2016. Toxicol Pathol 44, 1072–1083.
PMID: 27638646; PMCID: PMC5330931 -
Krischke, M., Hempel, G., Völler, S., André, N., D’Incalci, M., Bisogno, G., Köpcke, W., Borowski, M., Herold, R., Boddy, A.V., Boos, J., 2016. Cancer Chemother Pharmacol 78, 1175–1184.
-
Meluzin, J., Starek, Z., Kulik, T., Jez, J., Lehar, F., Tomandl, J., Dusek, L., Wolf, J., Leinveber, P., Novak, M., 2016. Echocardiography 34, 78–86.
-
Niccoli, G., Conte, M., Marchitti, S., Montone, R.A., Fracassi, F., Grippo, R., Roberto, M., Burzotta, F., Trani, C., Leone, A.M., Bianchi, F., Di Castro, S., Volpe, M., Crea, F., Rubattu, S., 2016. Cardiovasc Revasc Med 17, 162–168.
PMID: 26987266 -
ProANP as a screening biomarker for hypertrophic cardiomyopathy in Maine coon cats.
Parzeniecka-Jaworska, M., Garncarz, M., Kluciński, W., 2016. Polish Journal of Veterinary Sciences 19, 801–807.
-
Stanciu, A.E., Hurduc, A.E., Stanciu, M.M., 2016. Scandinavian Journal of Clinical and Laboratory Investigation 76, 626–631.
PMID: 27666870 -
Cross-laboratory analytical validation of the cardiac biomarker NT-proANP in rat
Vinken, P., Reagan, W.J., Rodriguez, L.A., Buck, W.R., Lai-Zhang, J., Goeminne, N., Barbacci, G., Liu, R., King, N.M.P., Engle, S.K., Colton, H., 2016. Journal of Pharmacological and Toxicological Methods 77, 58–65.
-
Novel MicroRNA Regulators of Atrial Natriuretic Peptide Production.
Wu, C., Arora, P., Agha, O., Hurst, L.A., Allen, K., Nathan, D.I., Hu, D., Jiramongkolchai, P., Smith, J.G., Melander, O., Trenson, S., Janssens, S.P., Domian, I., Wang, T.J., Bloch, K.D., Buys, E.S., Bloch, D.B., Newton-Cheh, C., 2016. Mol. Cell. Biol. 36, 1977–1987.
PMID: 27185878; PMCID: PMC4936060 -
Weight loss, saline loading, and the natriuretic peptide system.
Arora, P., Reingold, J., Baggish, A., Guanaga, D.P., Wu, C., Ghorbani, A., Song, Y., Chen-Tournaux, A., Khan, A.M., Tainsh, L.T., Buys, E.S., Williams, J.S., Heublein, D.M., Burnett, J.C., Semigran, M.J., Bloch, K.D., Scherrer-Crosbie, M., Newton-Cheh, C., Kaplan, L.M., Wang, T.J., 2015. J Am Heart Assoc 4, e001265.
PMID: 25595796; PMCID: PMC4330054 -
Increased plasma corin levels in patients with atrial fibrillation.
Chen, F., Xia, Y., Liu, Y., Zhang, Y., Song, W., Zhong, Y., Gao, L., Jin, Y., Li, S., Jiang, Y., Yang, Y., 2015. Clinica Chimica Acta 447, 79–85.
-
Lee, J.S., Ko, Y.-G., Shin, K.-J., Kim, S.-K., Park, J.H., Hwang, K.-C., Pak, H.-N., 2015. Yonsei Medical Journal 56, 53–61.
-
Natriuretic peptides for the detection of paroxysmal atrial fibrillation.
Seegers, J., Zabel, M., Grüter, T., Ammermann, A., Weber-Krüger, M., Edelmann, F., Gelbrich, G., Binder, L., Herrmann-Lingen, C., Gröschel, K., Hasenfuß, G., Feltgen, N., Pieske, B., Wachter, R., 2015. Open Heart 2.
PMID: 26288739; PMCID: PMC4533200 -
Shurupov, V., Suslova, T., Ryabov, V., 2015. AIP Conference Proceedings 1688, 060008.
-
Stokes, A.H., Falls, J.G., Yoon, L., Cariello, N., Faiola, B., Colton, H.M., Jordan, H.L., Berridge, B.R., 2015. Int J Toxicol 34, 151–161.
-
Renal Mechanisms of Association between Fibroblast Growth Factor 1 and Blood Pressure.
Tomaszewski, M., Eales, J., Denniff, M., Myers, S., Chew, G.S., Nelson, C.P., Christofidou, P., Desai, A., Büsst, C., Wojnar, L., Musialik, K., Jozwiak, J., Debiec, R., Dominiczak, A.F., Navis, G., van Gilst, W.H., van der Harst, P., Samani, N.J., Harrap, S., Bogdanski, P., Zukowska-Szczechowska, E., Charchar, F.J., 2015. J Am Soc Nephrol 26, 3151–3160.
PMID: 25918036; PMCID: PMC4657842 -
Novel biomarkers for risk stratification in pulmonary arterial hypertension.
Zelniker, T., Uhlmann, L., Spaich, S., Friedrich, J., Preusch, M.R., Meyer, F.J., Katus, H.A., Giannitsis, E., 2015. ERJ Open Res 1.
PMID: 27730146; PMCID: PMC5005111 -
Bergmann, A., Papassotiriou, J., Struck, J., Morgenthaler, N., Anker, S., 2014. US8647830B2
-
Krag, A., Bendtsen, F., Dahl, E.K., Kjær, A., Petersen, C.L., Møller, S., 2014. PLOS ONE 9, e109179.
-
Essential role of sympathetic endothelin A receptors for adverse cardiac remodeling.
Lehmann, L.H., Rostosky, J.S., Buss, S.J., Kreusser, M.M., Krebs, J., Mier, W., Enseleit, F., Spiger, K., Hardt, S.E., Wieland, T., Haass, M., Lüscher, T.F., Schneider, M.D., Parlato, R., Gröne, H.-J., Haberkorn, U., Yanagisawa, M., Katus, H.A., Backs, J., 2014. Proc Natl Acad Sci U S A 111, 13499–13504.
PMID: 25197047; PMCID: PMC4169911 -
Li, A.M., Au, C.T., Zhu, J., Chan, K., Chan, M., Lee, D., Wing, Y.K., 2014. Front. Pediatr. 2.
-
Cardiovascular risk markers in dilated cardiomyopathy in Emery–Dreifuss muscular dystrophy (EDMD).
Niebroj-Dobosz, I., Sokołowska, B., Madej-Pilarczyk, A., Marchel, M., Hausmanowa-Petrusewicz, I., 2014. International Journal of Cardiology 173, 324–325.
PMID: 24681014 -
Zavadovsky, K.V., Krivonogov, N.G., Lishmanov, Y.B., 2014. Ann Nucl Med 28, 632–637.
-
Zhang, Yue, Li, H., Zhou, J., Wang, A., Yang, J., Wang, C., Liu, M., Zhou, T., Zhu, L., Zhang, Yonghong, Dong, N., Wu, Q., 2014. Scientific Reports 4, 7378.
-
Bacaksiz, A., Vatankulu, M.A., Kayrak, M., Telli, H.H., Ayhan, S.S., Sonmez, O., Alp, A., Buyukbas, S., 2013. Clinics (Sao Paulo) 68, 997–1003.
PMID: 23917666; PMCID: PMC3714741 -
Natriuretic peptide fragments as possible biochemical markers of hypertension in the elderly.
Cappellin, E., Gatti, R., Antonelli, G., Soldà, G., Ragazzi, E., Palo, E.F.D., Spinella, P., 2013. Journal of Cardiovascular Medicine 14, 308.
-
Kostopoulou, A.G., Tsiapras, D.P., Chaidaroglou, A.S., Giannis, D.E.D., Farmakis, D., Kremastinos, D.T., 2013. American Journal of Hematology 89, 13–18.
-
Magrì, D., Agostoni, P., Ricotta, A., Pisani, L., Cauti, F.M., Onofri, A., Bruno, P., Ricci, A., Volpe, M., Marchitti, S., Mariotta, S., Rubattu, S., 2013. European Journal of Internal Medicine 24, 278–284.
-
Meluzin, J., Hude, P., Krejci, J., Spinarova, L., Podrouzkova, H., Leinveber, P., Dusek, L., Soska, V., Tomandl, J., Nemec, P., 2013. Exp Clin Cardiol 18, 63–72
PMID: 23940422; PMCID: PMC3718577 -
Pizon, Marek, Friedel, N., Pizon, Monika, Freundt, M., Weyand, M., Feyrer, R., 2013. Journal of Cardiothoracic Surgery 8, 218.
-
Stahrenberg, R., Niehaus, C.-F., Edelmann, F., Mende, M., Wohlfahrt, J., Wasser, K., Seegers, J., Hasenfuß, G., Gröschel, K., Wachter, R., 2013. J. Neurol. Neurosurg. Psychiatry 84, 479–487.
PMID: 23355808; PMCID: PMC3623028 -
Natriuretic peptide proANP (1-98), a biomarker of ALI/ARDS in burns.
Tokarik, M., Sjöberg, F., Vajtr, D., Broz, L., Balik, M., Vranova, J., 2013. Burns 39, 243–248.
PMID: 23006832 -
Wiedemann, S., Wessela, T., Schwarz, K., Joachim, D., Jercke, M., Strasser, R.H., Ebner, B., Simonis, G., 2013. Mol Cell Biochem 372, 275–283.
-
Wolf, J., Gerlach, N., Weber, K., Klima, A., Wess, G., 2013. Veterinary Clinical Pathology 42, 196–206.
-
NT-proANP circulating level is a prognostic marker in stable ischemic heart disease.
Barbato, E., Bartunek, J., Marchitti, S., Mangiacapra, F., Stanzione, R., Delrue, L., Cotugno, M., Di, S.C., De, B.B., Wijns, W., Volpe, M., Rubattu, S., Rubattu, S., 2012. Int J Cardiol 155, 311–312.
PMID: 22177588 -
Cabiati, M., Caruso, R., Caselli, C., Frigerio, M., Prescimone, T., Parodi, O., Giannessi, D., Del Ry, S., 2012. Peptides 36, 192–198.
-
Neurohormonal and cytokine fluctuations following transcatheter closure for an atrial septal defect.
Chamakou, A.C., Dede, E., Moutafi, A., Thanopoulos, V., Chryssanthopoulos, S., Loukopoulou, S., Pitsavos, C., Stefanadis, C., Davos, C.H., 2012. Cytokine 57, 130–135.
-
Atrial natriuretic peptides in Han Wistar, Sprague-Dawley and spontaneously hypertensive rats.
Crivellente, F., Bocchini, N., Bonato, M., Vandin, L., Faustinelli, I., Cristofori, P., 2012. J Appl Toxicol 32, 521–526.
PMID: 22083722 -
Govindan, M., Borgulya, G., Kiotsekoglou, A., Saha, S.K., Camm, A.J., 2012. Europace 14, 1302–1310.
PMID: 22654096 -
Does the Relationship Between Natriuretic Hormones and Diastolic Function Differ by Race?
Kapuku, G.K., Davis, H.C., Harshfield, G.A., Thomas, P., Januzzi, J., 2012. The American Journal of the Medical Sciences 344, 96–99.
-
Kristensen, T., Urke, H.A., Poppe, T.T., H.Takle, 2012. Aquaculture, Smolt 2009: Proceedings of the 8th International Workshop on Smoltification. 362–363, 172–176.
-
Madziarska, K., Weyde, W., Krajewska, M., Szczechowska, E.Z., Gosek, K., Penar, J., Klak, R., Golebiowski, T., Kozyra, C., Klinger, M., 2012. Int Urol Nephrol 44, 955–961.
-
Natriuretic Peptide Concentrations in Centenarians.
Nybo, M., Jeune, B., Andersen‐Ranberg, K., 2012. Journal of the American Geriatrics Society 60, 991–993.
-
Mechanism of stretch-induced activation of the mechanotransducer zyxin in vascular cells.
Suresh Babu, S., Wojtowicz, A., Freichel, M., Birnbaumer, L., Hecker, M., Cattaruzza, M., 2012. Sci Signal 5, ra91.
PMID: 23233529 -
Uhm, J.-S., Mun, H.-S., Wi, J., Shim, J., Joung, B., Lee, M.-H., Pak, H.-N., 2012. Pacing and Clinical Electrophysiology 36, 163–171.
-
Wachter, R., Lahno, R., Haase, B., Weber-Krüger, M., Seegers, J., Edelmann, F., Wohlfahrt, J., Gelbrich, G., Görlitz, A., Kermer, P., Vollmann, D., Hasenfuß, G., Gröschel, K., Stahrenberg, R., 2012. PLOS ONE 7, e34351.
-
Wilhelm, Matthias, Nuoffer, J.-M., Schmid, J.-P., Wilhelm, I., Saner, H., 2012. The American Journal of Cardiology 109, 1060–1065.
-
Inflammation and atrial remodeling after a mountain marathon.
Wilhelm, M., Zueger, T., Marchi, S.D., Rimoldi, S.F., Brugger, N., Steiner, R., Stettler, C., Nuoffer, J.-M., Seiler, C., Ith, M., 2012. Scandinavian Journal of Medicine & Science in Sports 24, 519–525.
-
Zaki, M.A., El-Banawy, S.E.-D.S., El-Gammal, H.H., 2012. Pregnancy Hypertension: An International Journal of Women’s Cardiovascular Health 2, 48–52.
-
Barbato, A., Strazzullo, P., Volpe, M., Rubattu, S., 2011. Journal of Thrombosis and Haemostasis 9, 1662–1663.
-
Colton, H.M., Stokes, A.H., Yoon, L.W., Quaile, M.P., Novak, P.J., Falls, J.G., Kimbrough, C.L., Cariello, N.F., Jordan, H.L., Berridge, B.R., 2011. Toxicol. Sci. 120, 262–268.
PMID: 21242511 -
den Uijl, D.W., Delgado, V., Tops, L.F., Ng, A.C.T., Boersma, E., Trines, S.A., Zeppenfeld, K., Schalij, M.J., van der Laarse, A., Bax, J.J., 2011. American Heart Journal 161, 197–203.
-
Dineva, J., Vangelov, I., Nikolov, G., Gulenova, D., Ivanova, M., 2011. Journal of Obstetrics and Gynaecology Research 37, 511–519.
-
Gole, Y., Gargne, O., Coulange, M., Steinberg, J.-G., Bouhaddi, M., Jammes, Y., Regnard, J., Boussuges, A., 2011. Eur J Appl Physiol 111, 937–946.
-
Mechanism of 1-deamino-arginine vasotocin induced natriuresis in rats.
Karavashkina, T.A., Kutina, A.V., Shakhmatova, E.I., Natochin, Y.V., 2011. General and Comparative Endocrinology 170, 460–467.
-
Krogh, J., Ströhle, A., Westrin, Å., Klausen, T., Jørgensen, M.B., Nordentoft, M., 2011. Psychoneuroendocrinology 36, 656–663.
-
Lipid-apheresis improves microcirculation of the upper limbs.
Rossenbach, J., Mueller, G.A., Lange, K., Armstrong, V.W., Schmitto, J.D., Hintze, E., Helfmann, J., Konstantinides, S., Koziolek, M.J., 2011. Journal of Clinical Apheresis 26, 167–173.
-
Cao, H., Xue, L., Wu, Y., Ma, H., Chen, L., Wang, X., Zhu, Q., Dai, N., Chen, Y., 2010. Peptides 31, 1531–1539.
-
N-Terminal Pro C-Type Natriuretic Peptide Relation With Prolactin in the Elderly.
Cappellin, E., Spinella, P., Antonelli, G., Gatti, R., Soldà, G., De Palo, E.F., 2010. The Endocrinologist 20, 185–189.
-
Engle, S.K., Solter, P.F., Credille, K.M., Bull, C.M., Adams, S., Berna, M.J., Schultze, A.E., Rothstein, E.C., Cockman, M.D., Pritt, M.L., Liu, H., Lu, Y., Chiang, A.Y., Watson, D.E., 2010. Toxicol. Sci. 114, 183–192.
PMID: 20044590 -
Gutte, H., Mortensen, J., Jensen, C.V., Recke, P.V.D., Petersen, C.L., Kristoffersen, U.S., Kjær, A., 2010. Clinical Physiology and Functional Imaging 30, 466–472.
-
Kemter, E., Rathkolb, B., Bankir, L., Schrewe, A., Hans, W., Landbrecht, C., Klaften, M., Ivandic, B., Fuchs, H., Gailus-Durner, V., Hrabé de Angelis, M., Wolf, E., Wanke, R., Aigner, B., 2010. Am. J. Physiol. Renal Physiol. 298, F1405-1415.
PMID: 20219826 -
Serological Predictors for the Recurrence of Atrial Fibrillation After Electrical Cardioversion.
Kim, S.K., Pak, H.-N., Park, J.H., Ko, K.J., Lee, J.S., Wi, J., Choi, J.I., Kim, Y.-H., 2010. Korean Circ J 40, 185–190.
PMID: 20421959; PMCID: PMC2859336
-
Ultrasonic evidence of acute interstitial lung edema after SCUBA diving is resolved within 2–3h.
Ljubkovic, M., Gaustad, S.E., Marinovic, J., Obad, A., Ivancev, V., Bilopavlovic, N., Breskovic, T., Wisloff, U., Brubakk, A., Dujic, Z., 2010. Respiratory Physiology & Neurobiology 171, 165–170.
-
Møller, S., Iversen, J.S., Krag, A., Bie, P., Kjaer, A., Bendtsen, F., 2010. Am. J. Physiol. Gastrointest. Liver Physiol. 299, G784-790.
PMID: 20616307 -
Sachidhanandam, M., Singh, S.N., Salhan, A.K., Ray, U.S., 2010. Indian J Clin Biochem 25, 153–157.
-
Plasma proANP1-98 Response During High Altitude Stress: Effect of Age and Ethnicity.
Sachidhanandam, Meenakshi, Singh, S.N., Sharma, Y.K., Salhan, A.K., Ray, U.S., 2010. Wilderness & Environmental Medicine 21, 11–16.
-
BNP controls early load-dependent regulation of SERCA through calcineurin.
Toischer, K., Teucher, N., Unsöld, B., Kuhn, M., Kögler, H., Hasenfuss, G., 2010. Basic Res Cardiol 105, 795–804.
-
Zimmering, T.M., Hungerbühler, S., Meneses, F., Nolte, I., Simon, D., 2010. Journal of the American Veterinary Medical Association 237, 665–672.
-
Андреева, Ю.А., Саидова, М.А., Мартынюк, Т.В., Масенко, В.П., Чазова, И.Е., 2010. Кардиоваскулярная терапия и профилактика.
-
Hammerer-Lercher, A., Sommer, R., Mair, J., Tulzer, G., Lechner, E., Hawa, G., Maitzen, S., Woloszczuk, W., Puschendorf, B., 2008. Clinica Chimica Acta 391, 118–119.
-
Paniagua, R., Amato, D., Mujais, S., Vonesh, E., Ramos, A., Correa-Rotter, R., Horl, W.H., 2008. Clin J Am Soc Nephrol 3, 407–415.
PMID: 18199844; PMCID: PMC2390944 -
Sharma, V., Dhillon, P., Wambolt, R., Parsons, H., Brownsey, R., Allard, M.F., McNeill, J.H., 2008. Am. J. Physiol. Heart Circ. Physiol. 294, H1609-1620.
PMID: 18203848 -
Assmus, B., Fischer-Rasokat, U., Honold, J., Seeger, F.H., Fichtlscherer, S., Tonn, T., Seifried, E., Schächinger, V., Dimmeler, S., Zeiher, A.M., TOPCARE-CHD Registry, 2007. Circ. Res. 100, 1234–1241.
PMID: 17379833 -
Galasko, G., Collinson, P.O., Barnes, S.C., Gaze, D., Lahiri, A., Senior, R., 2007. J. Clin. Pathol. 60, 570–572.
PMID: 17513518; PMCID: PMC1994520 -
Sin, D.D., Wong, E., Mayers, I., Lien, D.C., Feeny, D., Cheung, H., Gan, W.Q., Man, S.F.P., 2007. Chest 131, 156–163.
PMID: 17218570 -
Reduced apelin levels in lone atrial fibrillation.
Ellinor, P.T., Low, A.F., Macrae, C.A., 2006. Eur. Heart J. 27, 222–226.
PMID: 16278229 -
Linz, W., Schäfer, S., Afkham, F., Gerl, M., Schmidts, H.-L., Rütten, H., 2006. J Renin Angiotensin Aldosterone Syst 7, 155–161.
PMID: 17094052 -
Rubattu, S., Bigatti, G., Evangelista, A., Lanzani, C., Stanzione, R., Zagato, L., Manunta, P., Marchitti, S., Venturelli, V., Bianchi, G., Volpe, M., Stella, P., 2006. J. Am. Coll. Cardiol. 48, 499–505.
PMID: 16875975 -
Apoptosis at a distance: remote activation of caspase-3 occurs early after myocardial infarction.
Schwarz, K., Simonis, G., Yu, X., Wiedemann, S., Strasser, R.H., 2006. Mol. Cell. Biochem. 281, 45–54.
PMID: 16328956 -
Staudt, A., Staudt, Y., Hummel, A., Empen, K., Dörr, M., Trimpert, C., Birkenmeier, K., Kühl, U., Noutsias, M., Russ, D., Felix, S.B., 2006. Ther Apher Dial 10, 42–48.
PMID: 16556135 -
Toma, I., Sax, B., Nagy, A., Entz, L., Rusvai, M., Juhász-Nagy, A., Kékesi, V., 2006. Exp. Biol. Med. (Maywood) 231, 847–851
PMID: 16741010 -
Windt, W.A.K.M., Eijkelkamp, W.B.A., Henning, R.H., Kluppel, A.C.A., de Graeff, P.A., Hillege, H.L., Schäfer, S., de Zeeuw, D., van Dokkum, R.P.E., 2006. J. Am. Soc. Nephrol. 17, 3059–3066.
PMID: 17005935 -
Yilmaz, M.B., Erbay, A.R., Balci, M., Guray, Y., Cihan, G., Guray, U., Kisacik, H.L., Korkmaz, S., 2006. Cardiology 105, 207–212.
PMID: 16498244 -
Berger, R., Huelsmann, M., Strecker, K., Moertl, D., Moser, P., Bojic, A., Pacher, R., 2005. Eur. J. Clin. Invest. 35, 24–31.
PMID: 15638816 -
Prognostic value of plasma N-terminal pro-brain natriuretic peptide in patients with severe sepsis.
Brueckmann, M., Huhle, G., Lang, S., Haase, K.K., Bertsch, T., Weiss, C., Kaden, J.J., Putensen, C., Borggrefe, M., Hoffmann, U., 2005. Circulation 112, 527–534.
PMID: 16027260 -
Ellinor, P.T., Low, A.F., Patton, K.K., Shea, M.A., Macrae, C.A., 2005. J. Am. Coll. Cardiol. 45, 82–86.
PMID: 15629379 -
Hoffmann, U., Brueckmann, M., Bertsch, T., Wiessner, M., Liebetrau, C., Lang, S., Haase, K.K., Borggrefe, M., Huhle, G., 2005. Clin. Lab. 51, 373–379
PMID: 16122147 -
Hülsmann, M., Berger, R., Mörtl, D., Gore, O., Meyer, B., Pacher, R., 2005. Eur. J. Heart Fail. 7, 552–556.
PMID: 15921794 -
Jarai, Rudolf, Iordanova, N., Jarai, Robert, Raffetseder, A., Woloszczuk, W., Gyöngyösi, M., Geyer, G., Wojta, J., Huber, K., 2005. Eur. Heart J. 26, 250–256.
PMID: 15618049 -
Serum atrial natriuretic peptide levels in infants with transient tachypnea of the newborn.
Onal, E.E., Dilmen, U., Adam, B., Türkyilmaz, C., Uysal, F.K., Oğuz, D., 2005. J. Matern. Fetal. Neonatal. Med. 17, 145–149.
PMID: 16076624 -
Rosolova, H., Cech, J., Simon, J., Spinar, J., Jandova, R., Widimský sen, J., Holubec, L., Topolcan, O., 2005. Eur. J. Heart Fail. 7, 780–783.
PMID: 16051521 -
Bergler-Klein, J., Klaar, U., Heger, M., Rosenhek, R., Mundigler, G., Gabriel, H., Binder, T., Pacher, R., Maurer, G., Baumgartner, H., 2004. Circulation 109, 2302–2308.
PMID: 15117847 -
Collinson, P.O., Barnes, S.C., Gaze, D.C., Galasko, G., Lahiri, A., Senior, R., 2004. European Journal of Heart Failure 6, 365–368.
-
Natriuretic peptides and the prevalence of congestive heart failure in patients with pacemakers.
Gwechenberger, M., Huelsmann, M., Graf, S., Berger, R., Bonderman, D., Stanek, B., Rauscha, F., Pacher, R., 2004. Eur. J. Clin. Invest. 34, 811–817.
PMID: 15606723 -
Hammerer-Lercher, A., Ludwig, W., Falkensammer, G., Müller, S., Neubauer, E., Puschendorf, B., Pachinger, O., Mair, J., 2004. Clinical Chemistry 50, 1174–1183.
PMID: 15142976 -
Hoffmann, U., Brückmann, M., Liebetrau, C., Lang, S., Bertsch, T., Borggrefe, M., Putensen, C., Schröder, S., Haase, K., 2004. Crit Care 8, P113.
PMCID: PMC4099700 -
Muscle strength as a predictor of long-term survival in severe congestive heart failure.
Hülsmann, M., Quittan, M., Berger, R., Crevenna, R., Springer, C., Nuhr, M., Mörtl, D., Moser, P., Pacher, R., 2004. Eur. J. Heart Fail. 6, 101–107.
PMID: 15012925 -
Mazul-Sunko, B., Zarković, N., Vrkić, N., Antoljak, N., Bekavac Beslin, M., Nikolić Heitzler, V., Siranović, M., Krizmanić-Dekanić, A., Klinger, R., 2004. Nephron Clin Pract 97, 103-107.
PMID: 15292687 -
Atrial and brain natriuretic peptides as markers of response to resynchronisation therapy.
Molhoek, S.G., Bax, J.J., van Erven, L., Bootsma, M., Steendijk, P., Lentjes, E., Boersma, E., van der Laarse, A., van der Wall, E.E., Schalij, M.J., 2004. Heart 90, 97–98
PMID: 14676258; PMCID: PMC1768004 -
Patrianakos, A.P., Parthenakis, F.I., Papadimitriou, E.A., Diakakis, G.F., Tzerakis, P.G., Nikitovic, D., Vardas, P.E., 2004. Eur. J. Heart Fail. 6, 735–743.
PMID: 15542409 -
Goette, A., Jentsch-Ullrich, K., Lendeckel, U., Röcken, C., Agbaria, M., Auricchio, A., Mohren, M., Franke, A., Klein, H.U., 2003. Circulation. 8;108(20):2446-9.
PMID: 14610014 -
Mir, T.S., Laux, R., Hellwege, H.H., Liedke, B., Heinze, C., von Buelow, H., Läer, S., Weil, J., 2003. Pediatrics 112, 896–899
PMID: 14523183 -
Niessner, A., Ziegler, S., Slany, J., Billensteiner, E., Woloszczuk, W., Geyer, G., 2003. Eur. J. Endocrinol. 149, 555–559
PMID: 14640997 -
B-type natriuretic peptide predicts sudden death in patients with chronic heart failure.
Berger, R., Huelsman, M., Strecker, K., Bojic, A., Moser, P., Stanek, B., Pacher, R., 2002. Circulation 105, 2392–2397
PMID: 12021226 -
Hülsmann, M., Berger, R., Sturm, B., Bojic, A., Woloszczuk, W., Bergler-Klein, J., Pacher, R., 2002. Eur. Heart J. 23, 886–891.
PMID: 12042010 -
Amann, K., Simonaviciene, A., Medwedewa, T., Koch, A., Orth, S., Gross, M.L., Haas, C., Kuhlmann, A., Linz, W., Schölkens, B., Ritz, E., 2001. J. Am. Soc. Nephrol. 12, 2572–2584
PMID: 11729225 -
Clerico, A., Caprioli, R., Del Ry, S., Giannessi, D., 2001. J. Endocrinol. Invest. 24, 24–30.
PMID: 11227728 -
Franz, M., Woloszczuk, W., Hörl, W.H., 2001. Kidney Int. 59, 1928–1934.
PMID: 11318965 -
Hammerer-Lercher, A., Neubauer, E., Müller, S., Pachinger, O., Puschendorf, B., Mair, J., 2001. Clin. Chim. Acta 310, 193–197
PMID: 11498085 -
Early Post-Operative Haemodynamic and Neurohumoral Follow-Up After Endoaneurysmorrhaphy.
Jain, D, Grimm, M., Bartels, C., Bechtel, M., Tölg, R., Hartmann, F., Katus, H.A., Sievers, H.H., Richardt, G., 2001. Journal of Clinical and Basic Cardiology. 4 (2): 165-167
-
Jain, D., Schäfer, U., Dendorfer, A., Kurz, T., Lindemann, C., Tölg, R., Hartmann, F., Katus, H.A., Richardt, G., 2001. Indian Heart J 53, 301–307
PMID: 11516028 -
Mazul-Sunko, B., Zarkovic, N., Vrkic, N., Klinger, R., Peric, M., Bekavac-Beslin, M., Novkoski, M., Krizmanic, A., Gvozdenovic, A., Topic, E., 2001. J Endocrinol Invest 24, RC22–RC24.
-
Sandwich ELISA for proANP 1-98 facilitates investigation of left ventricular dysfunction.
Missbichler, A., Hawa, G., Schmal, N., Woloszczuk, W., 2001. Eur. J. Med. Res. 6, 105–111
PMID: 11309223 -
Retterstol, L., Djurovic, S., Bohn, M., Bakken, A., Erikssen, J., Berg, K., 2001. Scand. Cardiovasc. J. 35, 373–378
PMID: 11837516 -
Stanek, B., Frey, B., Hülsmann, M., Berger, R., Sturm, B., Strametz-Juranek, J., Bergler-Klein, J., Moser, P., Bojic, A., Hartter, E., Pacher, R., 2001. J. Am. Coll. Cardiol. 38, 436–442
PMID: 11499735 -
Clerico, A., Del Ry, S., Giannessi, D., 2000. Clin. Chem. 46, 1529–1534
PMID: 11017928
