 Download biomedica product list 2018
Download biomedica product list 2018Dickkopf-1 (DKK-1) ELISA

-
Category number
BI-20413
-
Method
Sandwich ELISA, HRP/TMB, 12×8-well detachable strips
-
Sample type
Serum
-
Sample volume
20 µl / well
-
Assay time
2 h / 1 h / 30 min
-
Sensitivity
1.7 pmol/l (= 43.0 pg/ml)
-
Standard range
0 – 160 pmol/l (= 0 – 4102 pg/ml)
-
Conversion factor
1 pg/ml = 0.039 pmol/l (MW: 25.8 kDa)
-
Precision
In-between-run (n=9): ≤3 % CV
Within-run (n=5): ≤ 3 % CV
-
Cross-reactivity
Human DKK-1 only, no cross-reactivity or interference with recombinant human DKK-2, DKK-4, Kremen-1, Kremen-2 or LRP-6 is observed.
-
Validation Data
See validation data tab for: precision, accuracy, diltuion linearity, values for healthy donors, etc.
-
Regulatory status
CE marked – for IVD use in the EU
Product overview
The DKK-1 immunoassay is a 3.5 hour, 96-well sandwich ELISA for the quantitative determination of DKK-1 in human serum. The assay employs human serum-based standards to ensure the measurement of biologically reliable data.
Principle of the Assay
The DKK-1 ELISA kit is a sandwich enzyme immunoassay for the quantitative determination of DKK-1 in human serum samples.
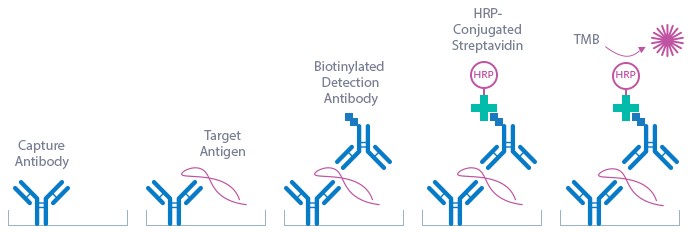
In a first step, assay buffer, standard/control/sample and detection antibody (biotinylated polyclonal rabbit anti-human DKK-1) are pipetted into the wells of the microtiter strips, which are pre-coated with monoclonal mouse anti-human DKK-1 antibody. DKK-1 present in the standard/control/sample binds to the pre-coated antibody in the well and forms a sandwich with the detection antibody. In the washing step all non-specific unbound material is removed. In a next step, the conjugate (streptavidin-HRP) is pipetted into the wells and reacts with the detection antibody. After another washing step, the substrate (TMB, tetramethylbenzidine) is pipetted into the wells. The enzyme-catalyzed color change of the substrate is directly proportional to the amount of DKK-1. This color change is detectable with a standard microtiter plate reader. A dose response curve of the absorbance (optical density, OD at 450 nm) versus standard concentration is generated using the values obtained from the standard. The concentration of DKK-1 in the sample is determined directly from the dose response curve.
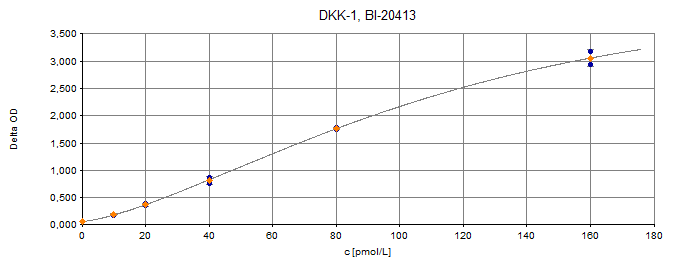
Typical Standard Curve
The figure below shows a typical standard curve for the DKK-1 ELISA. The immunoassay is calibrated against recombinant human DKK-1.
Kit Components
|
Contents |
Description |
Quantity |
|
PLATE |
Monoclonal mouse anti-human DKK-1 antibody pre-coated microtiter strips in strip holder packed in an aluminum bag with desiccant |
12 x 8 tests |
|
WASHBUF |
Wash buffer concentrate 20x, natural cap |
1 x 50 ml |
|
STD |
Standards 1-6, (0; 10; 20; 40; 80; 160 pmol/l), recombinant human DKK-1 in human serum, white caps, lyophilized |
6 vials |
|
CTRL |
Control, yellow cap, lyophilized, exact concentration after reconstitution see label |
1 vial |
|
ASYBUF |
Assay buffer, red cap, ready to use |
1 x 10 ml |
|
AB |
Polyclonal rabbit anti-human DKK-1 – biotin labeled, green cap, ready to use |
1 x 7 ml |
|
CONJ |
Conjugate (streptavidin-HRP), amber cap, ready to use |
1 x 13 ml |
|
SUB |
Substrate (TMB solution), amber bottle, blue cap, ready to use |
1 x 13 ml |
| STOP | STOP solution, white cap, ready to use | 1 x 7 ml |
Storage instructions: All reagents of the DKK-1 ELISA kit are stable at 2-8°C until the expiry date stated on the label of each reagent.
Serum is suitable for use in this assay. Do not change sample type during studies. We recommend duplicate measurements for all samples, standards and controls. The sample collection and storage conditions listed are intended as general guidelines.
Serum
Collect venous blood samples in standardized serum separator tubes (SST). Allow samples to clot for 30 minutes at room temperature. Perform separation by centrifugation according to the tube manufacturer’s instructions for use. Assay the acquired samples immediately or aliquot and store at -25°C or lower. Lipemic or hemolyzed samples may give erroneous results. Samples can undergo up to three freeze-thaw cycles.
Reagent Preparation
Wash Buffer
|
1. |
Bring the WASHBUF concentrate to room temperature. Crystals in the buffer concentrate will dissolve at room temperature. |
|
2. |
Dilute the WASHBUF concentrate 1:20, e.g. 50 ml WASHBUF + 950 ml distilled or deionized water. Only use diluted WASHBUF when performing the assay. |
The diluted WASHBUF is stable up to one month at 4°C (2-8°C).
Standards & Controls for Serum Measurements
|
1. |
Pipette 200 µl of distilled or deionized water into each standard (STD) and control (CTRL) vial. The exact concentration is printed on the label of each vial. |
|
2. |
Leave at room temperature (18-24°C) for 15 min. Swirl gently. |
Reconstituted STDs and CTRLs are stable at -25°C or lower until expiry date stated on the label. Avoid more than one freeze-thaw cycle.
Sample Preparation
Bring samples to room temperature and mix gently to ensure the samples are homogenous. We recommend duplicate measurements for all samples.
Samples for which the OD value exceeds he highest point of the standard range can be diluted with STD1 (standard 1).
Assay Protocol
Read the entire protocol before beginning the assay.
|
1. |
Bring samples and reagents to room temperature (18-24°C). |
|
2. |
Mark positions for STD/CTRL/SAMPLE (standard/control/sample) on the protocol sheet. |
|
3. |
Take microtiter strips out of the aluminum bag. Store unused strips with desiccant at 4°C in the aluminum bag. Strips are stable until expiry date stated on the label. |
|
4. |
Pipette 50 µl ASYBUF (assay buffer, red cap) into each well. |
|
5. |
Add 20 µl STD/CTRL/SAMPLE (standard/control/sample) in duplicates into the respective wells, swirl gently. |
|
6. |
Add 50 µl AB (biotinylated anti-DKK-1 antibody, green cap) into each well, swirl gently. |
|
7. |
Cover the plate tightly and incubate for 2 hours at room temperature (18-24°C). |
|
8. |
Aspirate and wash wells 5x with 300 µl diluted WASHBUF (wash buffer). After the final wash, remove remaining WASHBUF by strongly tapping the plate against a paper towel. |
|
9. |
Add 100 µl CONJ (conjugate, amber cap) into each well. |
|
10. |
Cover tightly and incubate for 1 hour at room temperature (18-24°C). |
|
11. |
Aspirate and wash wells 5x with 300 µl diluted WASHBUF (wash buffer). After the final wash, remove remaining WASHBUF by strongly tapping the plate against a paper towel. |
|
12. |
Add 100 µl SUB (substrate, blue cap) into each well. |
|
13. |
Incubate for 30 min at room temperature (18-24°C) in the dark. |
|
14. |
Add 50 µl STOP (stop solution, white cap) into each well, swirl gently. |
|
15. |
Measure absorbance immediately at 450 nm with reference 630 nm, if available. |
Calculation of Results
Read the optical density (OD) of all wells on a plate reader using 450 nm wavelength (reference wavelength 630 nm). Construct a standard curve from the absorbance read-outs of the standards using commercially available software capable of generating a four-parameter logistic (4-PL) fit. Alternatively, plot the standards’ concentration on the x-axis against the mean absorbance for each standard on the y-axis and draw a best fit curve through the points on the graph. Curve fitting algorithms other than 4-PL have not been validated and will need to be evaluated by the user.
Obtain sample concentrations from the standard curve. If required, pmol/l can be converted into pg/ml by applying a conversion factor (DKK-1: 1 pg/ml = 0.039 pmol/l; MW: 25.8 kDa). Respective dilution factors have to be considered when calculating the final concentration of the sample.
The quality control protocol supplied with the kit shows the results of the final release QC for each kit. ODs obtained by customers may differ due to various influences including a normal decrease of signal intensity throughout shelf life. However, this does not affect validity of results as long as an OD of 1.5 or higher is obtained for STD 6 and the value of the CTRL is within the target range (see label).
Information on the Analyte
DKK-1 is a 25.8 kDa secreted protein functioning as antagonist of the canonical Wnt signaling pathway. It is a member of the dickkopf-related protein family characterized by two cysteine-rich domains separated by a linker region. Binding of DKK-1 to the LRP5/6 co-receptor inhibits the interaction with Wnt and by forming a ternary complex with transmembrane Kremen-1 or -2, promotes the internalization of LRP5/6.
|
Molecular Weight |
25.8 kDa |
|
Cellular localization |
Extracellular |
|
Post-translational modifications |
Glycosylation |
|
Sequence similarities |
Member of the dickkopf-related protein family |
|
Alternative Names |
Dickkopf-1, DKK1, dickkopf WNT signaling pathway inhibitor, dickkopf (Xenopus laevis) homolog 1, dickkopf homolog 1 (Xenopus laevis), dickkopf related protein-1, dickkopf-related protein 1, SKdickkopf-1 like |
|
Entrez/NCBI ID |
22943 link: https://www.ncbi.nlm.nih.gov/gene/22943 |
|
Genecards |
GC10P052314 link: https://www.genecards.org/cgi-bin/carddisp.pl?gene=DKK1 |
|
OMIM |
605189 link: http://omim.org/entry/605189 |
|
Protein Atlas |
DKK1 link: https://www.proteinatlas.org/ENSG00000107984-DKK1/tissue |
|
Uniport ID |
O94907 (DKK1_HUMAN) link: https://www.uniprot.org/uniprot/O94907 |
The Wnt signaling pathway is involved in embryonic development, tissue differentiation and homeostasis as well as carcinogenesis. As soluble inhibitor of Wnt signaling, DKK-1 influences cell fate, proliferation, migration, polarity and gene expression.
Wnt signaling is particularly important in bone homeostasis as it induces the differentiation of osteoblasts while inhibiting osteoclastogenesis. DKK-1 is expressed in mature osteoblast and osteocytes and regulates the differentiation of osteoblasts. Thus, DKK-1 is centrally involved in the regulation of bone remodeling and its dysregulation is associated with bone pathologies.
Moreover, DKK-1 has emerged as a biomarker of cancer progression and prognosis as well as potential therapeutic target in various types of malignancies. In a range of different types of cancers, DKK-1 is further associated with formation of bone metastasis and osteolytic bone lesions.
-
Bone Disease
Osteoporosis
Rheumatoid arthritis
Ankylosing spondylitis
Axial spondyloarthritis
Osteoarthritis
Cancer-induced bone disease
Psoriatic arthritis
Primary hyperparathyroidism
Osteonecrosis
Osteopathy in type 1 diabetes
Osteogenesis imperfecta
-
Cancer
Breast cancer
Prostate cancer
Multiple myeloma
Cervical cancer
Hepatocellular carcinoma
Non-small cell lung cancer
Papillary thyroid cancer
Lung cancer
Bone metastasis
Cutaneous malignant melanoma
Monoclonal gammopathy of undetermined significance (MGUS)
Pancreatic ductal adenocarcinoma
Osteosarcoma
Chondrosarcoma
Esophageal squamous cell carcinoma
Papillary thyroid cancer
Bladder cancer
Gastric cancer
Colorectal cancer
Chronic lymphocytic leukemia
Pancreatic cancer
-
Cardiovascular disease
Abdominal aortic calcification
-
Other
Systemic mastocytosis
Nonalcoholic fatty liver disease
Type 2 Diabetes Mellitus
Anorexia nervosa
Acute infections
HIV-associated neurocognitive impairment
Literature
Molecular bases of the regulation of bone remodeling by the canonical Wnt signaling pathway.
Glass, D.A., Karsteny, G., 2006. Curr Top Dev Bio 73, 43-84.
![]() PMID: 16782455
PMID: 16782455
Wnt/β-catenin signaling: components, mechanisms, and diseases.
MacDonald, B.T., Tamai, K., He, X., 2009. Dev Cell 17, 9-26.![]() PMID: 19619488
PMID: 19619488
The emerging role of Dickkopf-1 in bone biology: is it the main switch controlling bone and joint remodeling?
Daoussis, D., Andonopoulos, A.P., 2011. Semin Arthritis Rheum 2, 170-177. ![]() PMID: 21435697
PMID: 21435697
Wnt signaling in cancer.
Zahn, T., Rindtorff, N., Boutros, M., 2017. Oncogene 36, 1461-1473.![]() PMID: 27617575
PMID: 27617575
Dickkopf-1 as a mediator and novel target in malignant bone disease.
Rachner, T.D., Göbel, A., Benad-Mehner, P., Hofbauer, L.C., Rauner, M., 2014. Cancer Lett 346, 172-177.![]() PMID: 24462802
PMID: 24462802
Rationale for targeting the Wnt signalling modulator Dickkopf-1 for oncology.
Kagey, M.H., He, X., 2017. Br J Pharmacol 174, 4637-4650.![]() PMID: 28574171
PMID: 28574171
Severe abdominal aortic calcification in older men is negatively associated with DKK1 serum levels: the STRAMBO study.
Szulc, P., Schoppet, M., Rachner, T.D., Chapurlat, R., Hofbauer, L.C., 2014. J Clin Endocrinol Metab 99, 617-624.![]() PMID: 24276456
PMID: 24276456
All Biomedica ELISAs are validated according to international FDA/ICH/EMEA guidelines. For more information about our validation guidelines, please refer to our quality page and published validation guidelines and literature.
1. ICH Q2(R1) Validation of Analytical Procedures: Text and Methodology
2. EMEA/CHMP/EWP/192217/2009 Guideline on bioanalytical method validation
3. Bioanalytical Method Validation, Guidance for Industry, FDA, May 2018
Calibration
The DKK-1 immunoassay is calibrated against recombinant DKK-1 protein (Uniprot ID O94907 (link: https://www.uniprot.org/uniprot/O94907)).
Detection Limit & Sensitivity
To determine the sensitivity of the DKK-1 ELISA, experiments measuring the lower limit of detection (LOD) and the lower limit of quantification (LLOQ) were conducted.
The LOD, also called the detection limit, is the lowest point at which a signal can be distinguished above the background signal, i.e. the signal that is measured in the absence of DKK-1, with a confidence level of 99%. It is defined as the mean back calculated concentration of standard 1 (0 pmol/l of DKK-1, five independent measurements) plus three times the standard deviation of the measurements.
The LLOQ, or sensitivity of an assay, is the lowest concentration at which an analyte can be accurately quantified. The criteria for accurate quantification at the LLOQ are an analyte recovery between 75 and 125% and a coefficient of variation (CV) of less than 25%. To determine the LLOQ, standard 2, i.e. the lowest standards containing DKK-1, is diluted, measured and its concentration back calculated. The lowest dilution, which meets both criteria, is reported as the LLOQ.
The following values were determined for the DKK-1 ELISA:
|
LOD |
1.7 pmol/l |
|
LLOQ |
1.25 pmol/l |
Precision
The precision of an ELISA is defined as its ability to measure the same concentration consistently within the same experiments carried out by one operator (within-run precision or repeatability) and across several experiments using the same samples but conducted by several operators at different locations using different ELISA lots (in-between-run precision or reproducibility).
Within-run (intra-assay precision) was assessed by measuring two samples of known concentration five times within one DKK-1 ELISA lot by one operator.
|
ID |
n |
Mean DKK-1 [pmol/l] |
SD [pmol/l] |
CV [%] |
|
S1 |
5 |
19.9 |
0.5 |
3 |
|
S2 |
5 |
80.1 |
2.7 |
3 |
In-between-run (inter-assay precision) was assessed by measuring two samples nine times within two DKK-1 ELISA kit lots by two different operators.
|
ID |
n |
Mean DKK-1 [pmol/l] |
SD [pmol/l] |
CV [%] |
|
S1 |
9 |
19.7 |
0.6 |
3 |
|
S2 |
9 |
80.4 |
2.1 |
3 |
Accuracy
The accuracy of an ELISA is defined as the precision with which it can recover samples of known concentrations.
The recovery of the DKK-1 ELISA was measured by adding recombinant DKK-1 to human samples containing a known concentration endogenous DKK-1. The % recovery of the spiked concentration was calculated as the percentage of measured compared over the expected value. All our ELISAs are expected to have % recovery rates within 15% of the nominal value of the sample.
This table shows the summary of the recovery experiments in the DKK-1 ELISA in serum matrix:
|
|
|
% Recovery |
|||
|
Sample Matrix |
n |
+40 pmol/l , DKK-1 |
+80 pmol/l, DKK-1 |
||
|
Mean |
Range |
Mean |
Range |
||
|
Serum |
7 |
93% |
86-103% |
96% |
87-106% |
Recovery of spiked samples was tested by adding two concentrations of human recombinant DKK-1 (40 pmol/l + 80 pmol/l) to human serum.
Data showing spike/recovery of human serum samples:
|
|
DKK-1 [pmol/l] |
% Recovery |
|||
|
Sample ID |
Reference |
+40 pmol/l |
+80 pmol/l |
+40 pmol/l |
+80 pmol/l |
|
#s1 |
6 |
43 |
88 |
96% |
103% |
|
#s2 |
10 |
38 |
79 |
86% |
87% |
|
#s3 |
12 |
43 |
82 |
92% |
94% |
|
#s4 |
29 |
50 |
90 |
93% |
92% |
|
#s5 |
41 |
57 |
98 |
93% |
92% |
|
#s6 |
50 |
61 |
104 |
92% |
95% |
|
#s7 |
61 |
70 |
122 |
103% |
106% |
|
Mean [%] |
93 |
96 |
|||
Dilution Linearity & Parallelism
Tests of dilution linearity and parallelism ensure that both endogenous and recombinant samples containing DKK-1 behave in a dose dependent manner and are not affected by matrix effects. Dilution linearity assesses the accuracy of measurements in diluted clinical samples spiked with known concentrations of recombinant analyte. By contrast, parallelism refers to dilution linearity in clinical samples and provides evidence that the endogenous analyte behaves in same way as the recombinant one. Dilution linearity and parallelism are assessed for each sample type and are acceptable if the results are within ±20% of the expected concentration.
Dilution linearity was assessed by serially diluting samples spiked with recombinant DKK-1 with STD1 (standard 1).
The table below shows the mean recovery and range of serially diluted recombinant DKK-1:
|
|
|
% Recovery of recombinant DKK-1 in diluted samples |
|||||
|
Sample Matrix |
n |
1+1 |
1+3 |
1+7 |
|||
|
Mean |
Range |
Mean |
Range |
Mean |
Range |
||
|
Serum |
3 |
106 |
91-116 |
102 |
93-109 |
102 |
100-105 |
|
DKK-1 [pmol/l] |
% Recovery |
|||||||
|
Sample matrix |
ID |
Reference |
1+1 |
1+3 |
1+7 |
1+1 |
1+3 |
1+7 |
|
Serum |
s1 |
80 |
36.2 |
16.8 |
8.6 |
91 |
93 |
102 |
|
Serum |
s2 |
94.2 |
54.5 |
29.8 |
15.0 |
116 |
109 |
100 |
|
Serum |
s3 |
135 |
75 |
37.1 |
19.5 |
111 |
99 |
105 |
|
|
Mean |
106 |
102 |
102 |
||||
|
|
Min |
91 |
93 |
100 |
||||
|
|
Max |
116 |
109 |
105 |
||||
Parallelism was assessed by serially diluting samples containing endogenous DKK-1 with with STD1 (standard 1).
The table below show the mean recovery and range of serially diluted endogenous DKK-1:
|
|
|
% Recovery of endogenous DKK-1 in diluted samples |
|||||
|
Sample Matrix |
n |
1+1 |
1+3 |
1+7 |
|||
|
Mean |
Range |
Mean |
Range |
Mean |
Range |
||
|
Serum |
4 |
109 |
108-112 |
104 |
99-107 |
100 |
90-114 |
|
DKK-1 [pmol/l] |
% Recovery |
|||||||
|
Sample matrix |
ID |
Reference |
1+1 |
1+3 |
1+7 |
1+1 |
1+3 |
1+7 |
|
Serum |
s1 |
51.8 | 28.5 | 14.8 | 8.4 | 110 | 103 | 114 |
|
Serum |
s2 |
30.2 | 16.3 | 8.7 | 3.9 | 108 | 107 | 90 |
|
Serum |
s3 |
47.6 | 26.5 | 14.0 | 6.6 | 112 | 106 | 95 |
|
Serum |
s4 |
42.8 | 23.1 | 11.4 | 5.7 | 108 | 99 | 100 |
| Mean | 109 | 104 | 100 | |||||
| Min | 108 | 99 | 90 | |||||
| Max | 110 | 107 | 114 | |||||
Specificity
The specificity of an ELISA is defined as its ability to exclusively recognize the analyte of interest.
The specificity of the ELISA was established through competition experiments, which measure the ability of the antibodies to exclusively bind DKK-1.
Competition of Signal
Competition experiments were carried out by pre-incubating human samples with an excess of coating antibody. The concentration measured in this mixture was then compared to a reference value, which was obtained from the same sample but without the pre-incubation step. The mean competition was 98%, demonstrating that this assay is specific for DKK-1.
|
DKK-1 [pmol/l] |
% Competition |
|||
|
Sample matrix |
ID |
Reference |
Reference + capture AB |
|
|
Serum |
s1 |
40 |
0 |
100 |
|
Serum |
s2 |
42 |
5 |
89 |
|
Serum |
s3 |
85 |
0 |
100 |
|
Serum |
s4 |
255 |
22 |
92 |
|
Serum |
s5 |
16 |
0 |
100 |
|
Serum |
s6 |
44 |
0 |
100 |
|
Serum |
s7 |
142 |
3 |
98 |
|
Serum |
s8 |
86 |
2 |
97 |
|
Serum |
s9 |
106 |
3 |
97 |
|
Serum |
s10 |
17 |
0 |
100 |
|
Serum |
s11 |
46 |
0 |
100 |
|
Serum |
s12 |
26 |
0 |
100 |
|
Serum |
s13 |
56 |
1 |
98 |
|
Serum |
s14 |
51 |
3 |
95 |
| Mean |
98 |
|||
Cross-Reactivity
The cross-reactivity of the DKK-1 ELISA was tested with recombinant DKK-2, which is 42% identical to DKK-1. The DKK-1 ELISA does not cross-react with DKK-2. No cross-reactivity or interference with recombinant human DKK-4, Kremen-1, Kremen-2 or LRP-6 is observed.
Sample Stability
The stability of endogenous DKK-1 was tested by comparing measurements in samples that had undergone six freeze-thaw cycles.
For freeze-thaw experiments, samples were collected according to the supplier’s instruction using blood collection devices and stored at -80°C. The mean recovery of sample concentration after an additional three freeze-thaw (F/T) cycles is 93%.
|
DKK-1 [pmol/l] |
% Recovery |
|||||
|
Sample matrix |
ID |
Reference |
3x F/T cycles |
6x F/T cycles |
3x F/T cycles |
6x F/T cycles |
|
Serum |
s1 |
43 |
40 |
40 |
93 |
92 |
|
Serum |
s2 |
70 |
63 |
62 |
90 |
89 |
|
Serum |
s3 |
46 |
46 |
43 |
94 |
93 |
|
Serum |
s4 |
21 |
21 |
19 |
96 |
88 |
|
Serum |
s5 |
30 |
30 |
31 |
100 |
103 |
|
Serum |
s6 |
41 |
39 |
38 |
95 |
91 |
|
Serum |
s7 |
29 |
26 |
27 |
89 |
92 |
|
Serum |
s8 |
46 |
43 |
40 |
92 |
87 |
|
Serum |
s9 |
152 |
139 |
131 |
91 |
86 |
|
Serum |
s10 |
106 |
99 |
93 |
94 |
88 |
|
Mean |
93 |
91 |
||||
All samples should undergo a maximum of three freeze-thaw cycles.
Sample Values
DKK-1 Values in Apparently Healthy Individuals
To provide expected values for circulating DKK-1, a panel of samples from apparently healthy donors was tested.
A summary of the results is shown below:
|
|
DKK-1 [pmol/l] |
||||
|
Sample Matrix |
n |
Mean |
Median |
Minimum |
Maximum |
|
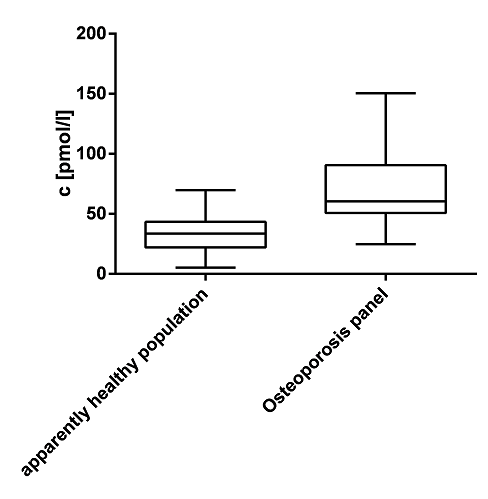
Serum |
51 |
35 |
34 |
5 |
70 |
We recommended establishing the normal range for each laboratory.
DKK-1 Values in an Osteoporosis Panel
In addition to samples from apparently healthy donors, a panel of samples from osteoporosis patients was tested.
A summary of the results is shown below:
|
|
DKK-1 [pmol/l] |
||||
|
Sample Matrix |
n |
Mean |
Median |
Minimum |
Maximum |
|
Serum |
48 |
69 |
60 |
25 |
150 |
A comparison of apparently healthy individuals and patients with osteoporosis shows that DKK-1 is increased in osteoporosis patients:
Automation
The assay was programmed on the ETI-Max3000. Standards and samples were tested and show a CV of <7% in the low to high calibration range. The coefficient of determination is >0.998 for a logit-log transformation.
An assay protocol for the ETI-max3000 is available on request.
-
-
Terpos, E., Katodritou, E., Symeonidis, A., Zagouri, F., Gerofotis, A., Christopoulou, G., Gavriatopoulou, M., Christoulas, D., Ntanasis-Stathopoulos, I., Kourakli, A., Konstantinidou, P., Kastritis, E., Dimopoulos, M.A., 2019. Int. J. Cancer.
 PMID: 30650184
PMID: 30650184 -
Valassi, E., García-Giralt, N., Malouf, J., Crespo, I., Llauger, J., Díez-Pérez, A., Webb, S.M., 2019. Endocr Connect 8, 39–49.
PMID: 30640713; PMCID: PMC6330718 - The serum sclerostin level is positively associated with the aortic augmentation index in patients on peritoneal dialysis.
Lin L., Yu-Hsien L., Liang-Te C., Jen-Pi T., Chih-Hsien W., Bang-Gee H., 2019. Tsu Chi Medical Journal -
Systemic Alterations of Wnt Inhibitors in Patients with Prostate Cancer and Bone Metastases.
Aufderklamm, S., Hennenlotter, J., Leidenberger, P., Rausch, S., Hohneder, A., Kühs, U., Maas, M., Schwentner, C., Bedke, J., Stenzl, A., Todenhöfer, T., 2018. Dis. Markers 2018, 1874598.
PMID: 30116403; PMCID: PMC6079590 -
LRP5 gene polymorphisms and radiographic joint damage in rheumatoid arthritis patients.
Bernardes, M., Durães, C., Oliveira, A., Martins, M.J., Lucas, R., Costa, L., Pereira, J.G., Ramos, I., Machado, J.C., Simões-Ventura, F., 2018. Osteoporosis International.
-
Bojanić, K., Bilić Ćurčić, I., Kuna, L., Kizivat, T., Smolic, R., Raguž Lučić, N., Kralik, K., Šerić, V., Ivanac, G., Tucak-Zorić, S., Včev, A., Smolić, M., 2018. J Clin Med 7.
PMID: 30227689; PMCID: PMC6162798 -
Boutsikas, G., Terpos, E., Papatheodorou, A., Tsirkinidis, P., Tsirigotis, P., Meletiou, A., Lalou, E., Telonis, V., Zannou, A., Kanellopoulos, A., Galani, Z., Stefanou, A., Tsaftaridis, P., Viniou, N.-A., Panayiotidis, P., Kyrtsonis, M.-C., Meletis, J., Vassilakopoulos, T.P., Angelopoulou, M.K., 2018. European Journal of Haematology 100, 131–139.
-
Catalano, A., Loddo, S., Bellone, F., Pecora, C., Lasco, A., Morabito, N., 2018. Bone 116, 42–46.
-
Chambard, L., Girard, N., Ollier, E., Rousseau, J.-C., Duboeuf, F., Carlier, M.-C., Brevet, M., Szulc, P., Pialat, J.-B., Wegrzyn, J., Clezardin, P., Confavreux, C.B., 2018. Bone 108, 202–209.
-
Chang, Y.-C., Hsu, B.-G., Liou, H.-H., Lee, C.-J., Wang, J.-H., 2018. BMC Cardiovasc Disord 18, 214.
PMID: 30482161 -
Fassio, A., Adami, G., Gatti, D., Orsolini, G., Giollo, A., Idolazzi, L., Benini, C., Vantaggiato, E., Rossini, M., Viapiana, O., 2018. Int. Immunopharmacol. 67, 487–489.
PMID: 30599401 -
Bone Geometry, Quality, and Bone Markers in Children with Type 1 Diabetes Mellitus.
Franceschi, R., Longhi, S., Cauvin, V., Fassio, A., Gallo, G., Lupi, F., Reinstadler, P., Fanolla, A., Gatti, D., Radetti, G., 2018. Calcified Tissue International 102, 657–665.
-
Gossiel, F., Scott, J.R., Paggiosi, M.A., Naylor, K.E., McCloskey, E.V., Peel, N.F.A., Walsh, J.S., Eastell, R., 2018. The Journal of Clinical Endocrinology & Metabolism 103, 1302–1309.
-
Bone metabolism in patients with anorexia nervosa and amenorrhoea.
Idolazzi, L., El Ghoch, M., Dalle Grave, R., Bazzani, P.V., Calugi, S., Fassio, S., Caimmi, C., Viapiana, O., Bertoldo, F., Braga, V., Rossini, M., Gatti, D., 2018. Eating and Weight Disorders - Studies on Anorexia, Bulimia and Obesity 23, 255–261.
-
Janjić, K., Cvikl, B., Kurzmann, C., Moritz, A., Agis, H., 2018. BMC Oral Health 18.
-
Kawazoe, M., Kaneko, K., Shikano, K., Kusunoki, N., Nanki, T., Kawai, S., 2018. Clinical Rheumatology 37, 2169–2178.
-
Rheumatoid arthritis in remission : Decreased myostatin and increased serum levels of periostin.
Kerschan-Schindl, K., Ebenbichler, G., Föeger-Samwald, U., Leiss, H., Gesslbauer, C., Herceg, M., Stummvoll, G., Marculescu, R., Crevenna, R., Pietschmann, P., 2018. Wien. Klin. Wochenschr.
PMID: 30171335 -
Myostatin and other musculoskeletal markers in lung transplant recipients.
Kerschan-Schindl, K., Ebenbichler, G., Gruther, W., Föger-Samwald, U., Kudlacek, S., Patsch, J., Gleiss, A., Jaksch, P., Klepetko, W., Pietschmann, P., 2018. Clin. Exp. Med.
PMID: 30317402 -
Lin, L., Lai, Y.-H., Chiu, L.-T., Tsai, J.-P., Wang, C.-H., Hsu, B.-G., 2018. Tzu Chi Medical Journal 0, 0.
-
DKK1 and sclerostin are early markers of relapse in multiple myeloma.
Mabille, C., Ruyssen-Witrand, A., Degboe, Y., Gennero, I., Loiseau, H.A., Roussel, M., Hebraud, B., Nigon, D., Attal, M., Laroche, M., 2018. Bone 113, 114–117.
-
Two-year cortical and trabecular bone loss in CKD-5D: biochemical and clinical predictors.
Malluche, H.H., Monier-Faugere, M.-C., Blomquist, G., Davenport, D.L., 2018. Osteoporosis International 29, 125–134.
-
Mantovani, A., Sani, E., Fassio, A., Colecchia, A., Viapiana, O., Gatti, D., Idolazzi, L., Rossini, M., Salvagno, G., Lippi, G., Zoppini, G., Byrne, C.D., Bonora, E., Targher, G., 2018. Diabetes Metab.
PMID: 30315891 -
Parathyroid hormone is a determinant of serum Dickkopf-1 levels in ankylosing spondylitis.
Orsolini, G., Adami, G., Rossini, M., Ghellere, F., Caimmi, C., Fassio, A., Idolazzi, L., Gatti, D., Viapiana, O., 2018. Clinical Rheumatology.
-
Differential effects of high-fat diet and exercise training on bone and energy metabolism.
Picke, A.-K., Sylow, L., Møller, L.L.V., Kjøbsted, R., Schmidt, F.N., Steejn, M.W., Salbach-Hirsch, J., Hofbauer, C., Blüher, M., Saalbach, A., Busse, B., Rauner, M., Hofbauer, L.C., 2018. Bone 116, 120–134.
-
Sun, W., Tian, L., Jiang, L., Zhang, S., Zhou, M., Zhu, J., Xue, J., 2018. Clin. Rheumatol.
PMID: 30443790 -
Terpos, E., Kastritis, E., Ntanasis-Stathopoulos, I., Christoulas, D., Papatheodorou, A., Eleutherakis-Papaiakovou, E., Kanellias, N., Fotiou, D., Ziogas, D.C., Migkou, M., Roussou, M., Trougkakos, I.P., Gavriatopoulou, M., Dimopoulos, M.A., 2018. Am. J. Hematol.
PMID: 30592079 -
Tsirkinidis, P., Terpos, E., Boutsikas, G., Papatheodorou, A., Anargyrou, K., Lalou, E., Dimitrakopoulou, A., Kalpadakis, C., Konstantopoulos, K., Siakantaris, M., Panayiotidis, P., Pangalis, G., Kyrtsonis, M.-C., Vassilakopoulos, T., Angelopoulou, M.K., 2018. Journal of Bone and Mineral Metabolism 36, 399–409.
-
-
Tsourdi, E., Makras, P., Rachner, T.D., Polyzos, S., Rauner, M., Mandanas, S., Hofbauer, L.C., Anastasilakis, A.D., 2018. Bone 120, 44–49.
PMID: 30292818 -
Wheater, G., Elshahaly, M., Naraghi, K., Tuck, S.P., Datta, H.K., van Laar, J.M., 2018. PLoS ONE 13, e0201527.
PMID: 30080871; PMCID: PMC6078302 -
Yang, H.-Y., Wu, D.-A., Chen, M.-C., Hsu, B.-G., 2018. Diab Vasc Dis Res 1479164118816661.
PMID: 30547685 -
Circulating levels of sclerostin but not DKK1 associate with laboratory parameters of CKD-MBD.
Behets, G.J., Viaene, L., Meijers, B., Blocki, F., Brandenburg, V.M., Verhulst, A., D’Haese, P.C., Evenepoel, P., 2017. PLOS ONE 12, e0176411.
-
Serum serotonin levels and bone in rheumatoid arthritis patients.
Bernardes, M., Vieira, T., Lucas, R., Pereira, J., Costa, L., Simões-Ventura, F., Martins, M.J., 2017. Rheumatology International 37, 1891–1898.
-
Bernardes, M., Vieira, T.S., Martins, M.J., Lucas, R., Costa, L., Pereira, J.G., Ventura, F., Martins, E., 2017. BioMed Research International 2017, 1–9.
-
Markers of bone metabolism during 14 days of bed rest in young and older men.
Buehlmeier, J., Frings-Meuthen, P., Mohorko, N., Lau, P., Mazzucco, S., Ferretti, J.L., Biolo, G., Pisot, R., Simunic, B., Rittweger, J., 2017. J Musculoskelet Neuronal Interact. 2017;17(1):399-408.
-
Wnt antagonist sclerostin and Dickkopf-1 in gestational diabetes.
Catalano, A., Pintaudi, B., Morabito, N., Giunta, L., Loddo, S., Corrado, F., D’Anna, R., Lasco, A., Di Benedetto, A., 2017. Diabetes & Metabolism 43, 375–377.
-
Serum levels of Dickkopf-1 are a potential negative biomarker of survival in geriatric patients.
Dovjak, P., Heinze, G., Rainer, A., Sipos, W., Pietschmann, P., 2017. Experimental Gerontology 96, 104–109.
-
In psoriatic arthritis Dkk-1 and PTH are lower than in rheumatoid arthritis and healthy controls.
Fassio, A., Idolazzi, L., Viapiana, O., Benini, C., Vantaggiato, E., Bertoldo, F., Rossini, M., Gatti, D., 2017. Clinical Rheumatology 36, 2377–2381.
-
Göbel, A., Kuhlmann, J.D., Link, T., Wimberger, P., Browne, A.J., Rauner, M., Hofbauer, L.C., Rachner, T.D., 2017. Breast Cancer Research and Treatment 164, 737–743.
-
Circulating Dickkopf-1 and sclerostin in patients with Paget’s disease of bone.
Idolazzi, L., Fassio, A., Tripi, G., Braga, V., Viapiana, O., Adami, G., Rossini, M., Gatti, D., 2017. Clinical Rheumatology 36, 925–928.
-
Effects of short-term dry immersion on bone remodeling markers, insulin and adipokines.
Linossier, M.-T., Amirova, L.E., Thomas, M., Normand, M., Bareille, M.-P., Gauquelin-Koch, G., Beck, A., Costes-Salon, M.-C., Bonneau, C., Gharib, C., Custaud, M.-A., Vico, L., 2017. PLOS ONE 12, e0182970.
-
Long-Term Effects of Severe Burn Injury on Bone Turnover and Microarchitecture.
Muschitz, G.K., Schwabegger, E., Fochtmann, A., Baierl, A., Kocijan, R., Haschka, J., Gruther, W., Schanda, J.E., Resch, H., Rath, T., Pietschmann, P., Muschitz, C., 2017. Journal of Bone and Mineral Research 32, 2381–2393.
-
Park, J.-H., Lee, S.-G., Jeon, Y.-K., Park, E.-K., Suh, Y.-S., Kim, H.-O., 2017. Medicine 96, e7854.
-
Effect of Tumor Necrosis Factor Inhibitor Therapy on Osteoclasts Precursors in Rheumatoid Arthritis.
Perpétuo, I.P., Caetano-Lopes, J., Rodrigues, A.M., Campanilho-Marques, R., Ponte, C., Canhão, H., Ainola, M., Fonseca, J.E., 2017. BioMed Research International 2017, 1–10.
-
Perpétuo, I.P., Caetano-Lopes, J., Vieira-Sousa, E., Campanilho-Marques, R., Ponte, C., Canhão, H., Ainola, M., Fonseca, J.E., 2017. Frontiers in Medicine 4.
-
Association between serum dickkopf-1 levels and disease duration in axial spondyloarthritis.
Rubio Vargas, R., Melguizo Madrid, E., González Rodríguez, C., Navarro Sarabia, F., Dominguez Quesada, C., Ariza Ariza, R., Navarro Compán, V., 2017. Reumatología Clínica 13, 197–200.
-
Serum dickkopf1 (DKK1), bone metabolism and atherosclerotic disease in patients with type 2 diabetes
Reyes-García R., Rozas-Moreno P., García-Martín A., García-Fontana B., Morales-Santana S., Muñoz-Torres M., 2017. Rev Osteoporos Metab Miner. 2016; 8 (1): 24-9
-
A Cytokine-Like Protein Dickkopf-Related Protein 3 Is Atheroprotective.
Yu, B., Kiechl, S., Qi, D., Wang, X., Song, Y., Weger, S., Mayr, A., Le Bras, A., Karamariti, E., Zhang, Z., Barco Barrantes, I. del, Niehrs, C., Schett, G., Hu, Y., Wang, W., Willeit, J., Qu, A., Xu, Q., 2017. Circulation 136, 1022–1036.
-
Higher Parathyroid Hormone Level Is Associated With Increased Arterial Stiffness in Type 1 Diabetes.
Zobel, E.H., Theilade, S., Scholten, B.J. von, Persson, F., Tarnow, L., Lajer, M., Hansen, T.W., Rossing, P., 2017. Diabetes Care 40, e32–e33.
PMID: 28062524 -
Adami, G., Orsolini, G., Adami, S., Viapiana, O., Idolazzi, L., Gatti, D., Rossini, M., 2016. Calcified Tissue International 99, 360–364.
-
Aschermann, S., Englbrecht, M., Bergua, A., Spriewald, B.M., Said-Nahal, R., Breban, M., Schett, G., Rech, J., 2016. Joint Bone Spine 83, 43–46.
-
Briot, K., Etcheto, A., Miceli-Richard, C., Dougados, M., Roux, C., 2016. Rheumatology 55, 335–342.
-
p38 MAPK regulates the Wnt inhibitor Dickkopf-1 in osteotropic prostate cancer cells.
Browne, A.J., Göbel, A., Thiele, S., Hofbauer, L.C., Rauner, M., Rachner, T.D., 2016. Cell Death & Disease 7, e2119–e2119.
-
Gómez-Vaquero, C., Martín, I., Loza, E., Carmona, L., Ivorra, J., Narváez, J.A., Hernández-Gañán, J., Alía, P., Narváez, J., 2016. PLOS ONE 11, e0166691.
-
Hsu, B.-G., Liou, H.-H., Lee, C.-J., Chen, Y.-C., Ho, G.-J., Lee, M.-C., 2016. Medicine 95, e3300.
-
Changes of serum sclerostin and Dickkopf-1 levels during the menstrual cycle. A pilot study.
Liakou, C.G., Mastorakos, G., Makris, K., Fatouros, I.G., Avloniti, A., Marketos, H., Antoniou, J.D., Galanos, A., Dontas, I., Rizos, D., Tournis, S., 2016. Endocrine 54, 543–551.
PMID: 27601021 -
Morabito, N., Catalano, A., Gaudio, A., Morini, E., Bruno, L.M., Basile, G., Tsiantouli, E., Bellone, F., Agostino, R.M., Piraino, B., La Rosa, M.A., Salpietro, C., Lasco, A., 2016. Journal of Bone and Mineral Metabolism 34, 540–546.
-
Muschitz, C., Kocijan, R., Haschka, J., Zendeli, A., Pirker, T., Geiger, C., Müller, A., Tschinder, B., Kocijan, A., Marterer, C., Nia, A., Muschitz, G.K., Resch, H., Pietschmann, P., 2016. Journal of Bone and Mineral Research 31, 672–682.
-
Circulating sclerostin and Dickkopf-1 levels in patients with nonalcoholic fatty liver disease.
Polyzos, S.A., Anastasilakis, A.D., Kountouras, J., Makras, P., Papatheodorou, A., Kokkoris, P., Sakellariou, G.T., Terpos, E., 2016. Journal of Bone and Mineral Metabolism 34, 447–456.
-
Rossini, M., Viapiana, O., Idolazzi, L., Ghellere, F., Fracassi, E., Troplini, S., Povino, M.R., Kunnathully, V., Adami, S., Gatti, D., 2016. Calcified Tissue International 98, 438–445.
-
Seror, R., Boudaoud, S., Pavy, S., Nocturne, G., Schaeverbeke, T., Saraux, A., Chanson, P., Gottenberg, J.-E., Devauchelle-Pensec, V., Tobón, G.J., Mariette, X., Miceli-Richard, C., 2016. Scientific Reports 6.
-
Valassi, E., Crespo, I., Malouf, J., Vilades, D., Leta, R., Llauger, J., Urgell, E., Aulinas, A., Marín, A.M., Biagetti, B., Webb, S.M., 2016. Endocrine 53, 860–864.
-
Briot, K., Rouanet, S., Schaeverbeke, T., Etchepare, F., Gaudin, P., Perdriger, A., Vray, M., Steinberg, G., Roux, C., 2015. Joint Bone Spine 82, 109–115.
-
Strong relationship between vitamin D status and bone mineral density in anorexia nervosa.
Gatti, D., El Ghoch, M., Viapiana, O., Ruocco, A., Chignola, E., Rossini, M., Giollo, A., Idolazzi, L., Adami, S., Dalle Grave, R., 2015. Bone 78, 212–215.
-
Gifre, L., Vidal, J., Carrasco, J.L., Filella, X., Ruiz-Gaspà, S., Muxi, A., Portell, E., Monegal, A., Guañabens, N., Peris, P., 2015. Journal of Bone and Mineral Research 30, 1014–1021.
-
Göbel, A., Browne, A.J., Thiele, S., Rauner, M., Hofbauer, L.C., Rachner, T.D., 2015. Breast Cancer Research and Treatment 154, 623–631.
-
Changes in Serum Levels of Myokines and Wnt-Antagonists after an Ultramarathon Race.
Kerschan-Schindl, K., Thalmann, M.M., Weiss, E., Tsironi, M., Föger-Samwald, U., Meinhart, J., Skenderi, K., Pietschmann, P., 2015. PLOS ONE 10, e0132478.
-
Lawrence, N.R., Jayasuriya, R.L., Gossiel, F., Wilkinson, J.M., 2015. HIP International 25, 525–530.
-
Malluche, H.H., Blomquist, G., Monier-Faugere, M.-C., Cantor, T.L., Davenport, D.L., 2015. Journal of the American Society of Nephrology 26, 2534–2544.
-
Sclerostin and DKK-1: two important regulators of bone metabolism in HIV-infected youths.
Mora, S., Puzzovio, M., Giacomet, V., Fabiano, V., Maruca, K., Capelli, S., Nannini, P., Lombardi, G., Zuccotti, G.V., 2015. Endocrine 49, 783–790.
-
Morena, M., Jaussent, I., Dupuy, A.-M., Bargnoux, A.-S., Kuster, N., Chenine, L., Leray-Moragues, H., Klouche, K., Vernhet, H., Canaud, B., Cristol, J.-P., 2015. Nephrology Dialysis Transplantation 30, 1345–1356.
-
Sclerostin Levels and Changes in Bone Metabolism After Bariatric Surgery.
Muschitz, C., Kocijan, R., Marterer, C., Nia, A.R., Muschitz, G.K., Resch, H., Pietschmann, P., 2015a. The Journal of Clinical Endocrinology & Metabolism 100, 891–901.
-
Muschitz, C., Kocijan, R., Pahr, D., Patsch, J.M., Amrein, K., Misof, B.M., Kaider, A., Resch, H., Pietschmann, P., 2015. Calcified Tissue International 96, 477–489.
-
Increase in Dickkopf-1 Serum Level in Recent Spondyloarthritis. Data from the DESIR Cohort.
Nocturne, G., Pavy, S., Boudaoud, S., Seror, R., Goupille, P., Chanson, P., van der Heijde, D., van Gaalen, F., Berenbaum, F., Mariette, X., Briot, K., Feydy, A., Claudepierre, P., Dieudé, P., Nithitham, J., Taylor, K.E., Criswell, L.A., Dougados, M., Roux, C., Miceli-Richard, C., 2015. PLOS ONE 10, e0134974.
-
Dickkopf-1 and sclerostin serum levels in patients with systemic mastocytosis.
Rossini, M., Viapiana, O., Zanotti, R., Tripi, G., Perbellini, O., Idolazzi, L., Bonifacio, M., Adami, S., Gatti, D., 2015. Calcif. Tissue Int. 96, 410–416.
PMID: 25694360 -
Serum fetuin-A levels and abdominal aortic calcification in healthy men — The STRAMBO study.
Schoppet, M., Rauner, M., Benner, J., Chapurlat, R., Hofbauer, L.C., Szulc, P., 2015. Bone 79, 196–202.
-
Yamada, S., Tsuruya, K., Tokumoto, M., Yoshida, H., Ooboshi, H., Kitazono, T., 2015. Nephrology 20, 639–645.
-
Yeremenko, N., Zwerina, K., Rigter, G., Pots, D., Fonseca, J.E., Zwerina, J., Schett, G., Baeten, D., 2015. Arthritis & Rheumatology 67, 2071–2075.
-
Downregulation of serum DKK-1 predicts poor prognosis in patients with papillary thyroid cancer.
Zhao, Y.P., Wang, W., Wang, X.H., Xu, Y., Wang, Y., Dong, Z.F., Zhang, J.J., 2015. Genetics and Molecular Research 14, 18886–18894.
-
Serum sclerostin in high-activity adult patients with juvenile idiopathic Arthritis.
Brabnikova-Maresova, K., Jarosova, K., Pavelka, K., Stepan, J.J., 2014. Arthritis Research & Therapy 16.
-
DKK-1 in prostate cancer diagnosis and follow up.
D’Amelio, P., Roato, I., Oderda, M., Soria, F., Zitella, A., Ferracini, R., Mengozzi, G., Gontero, P., Isaia, G.C., 2014. BMC Clinical Pathology 14.
-
Serum Levels of Sclerostin and Dickkopf-1: Effects of Age, Gender and Fracture Status.
Dovjak, P., Dorfer, S., Föger-Samwald, U., Kudlacek, S., Marculescu, R., Pietschmann, P., 2014. Gerontology 60, 493–501.
-
Foo, J.-P., Polyzos, S.A., Anastasilakis, A.D., Chou, S., Mantzoros, C.S., 2014. The Journal of Clinical Endocrinology & Metabolism 99, E2252–E2258.
-
Garcia-Martín, A., Reyes-Garcia, R., García-Fontana, B., Morales-Santana, S., Coto-Montes, A., Muñoz-Garach, M., Rozas-Moreno, P., Muñoz-Torres, M., 2014. PLoS ONE 9, e111703.
-
Gatti, D., Viapiana, O., Idolazzi, L., Fracassi, E., Ionescu, C., Dartizio, C., Troplini, S., Kunnathully, V., Adami, S., Rossini, M., 2014. Bone 67, 189–192.
Gaudio, A., Privitera, F., Pulvirenti, I., Canzonieri, E., Rapisarda, R., Fiore, C.E., 2014. Diabetes and Vascular Disease Research 11, 48–52
-
Klingberg, E., Nurkkala, M., Carlsten, H., Forsblad-d’Elia, H., 2014. The Journal of Rheumatology 41, 1349–1356.
-
Kyvernitakis, I., Rachner, T.D., Urbschat, A., Hars, O., Hofbauer, L.C., Hadji, P., 2014. Journal of Cancer Research and Clinical Oncology 140, 1671–1680.
-
Maïmoun, L., Guillaume, S., Lefebvre, P., Philibert, P., Bertet, H., Picot, M.-C., Gaspari, L., Paris, F., Courtet, P., Thomas, E., Mariano-Goulart, D., Bringer, J., Renard, E., Sultan, C., 2014. The Journal of Clinical Endocrinology & Metabolism 99, E582–E590.
-
Bone Mineral Density and Serum Biochemical Predictors of Bone Loss in Patients with CKD on Dialysis.
Malluche, H.H., Davenport, D.L., Cantor, T., Monier-Faugere, M.-C., 2014. Clinical Journal of the American Society of Nephrology 9, 1254–1262.
-
Dickkopf-1 is regulated by the mevalonate pathway in breast Cancer.
Rachner, T.D., Göbel, A., Thiele, S., Rauner, M., Benad-Mehner, P., Hadji, P., Bauer, T., Muders, M.H., Baretton, G.B., Jakob, F., Ebert, R., Bornhäuser, M., Schem, C., Hofbauer, L.C., 2014. Breast Cancer Research 16.
-
High serum levels of Dickkopf-1 are associated with a poor prognosis in prostate cancer patients.
Rachner, T.D., Thiele, S., Göbel, A., Browne, A., Fuessel, S., Erdmann, K., Wirth, M.P., Fröhner, M., Todenhöfer, T., Muders, M.H., Kieslinger, M., Rauner, M., Hofbauer, L.C., 2014. BMC Cancer 14
-
Simpson, C.A., Foer, D., Lee, G.S., Bihuniak, J., Sun, B., Sullivan, R., Belsky, J., Insogna, K.L., 2014. Osteoporosis International 25, 2383–2388.
-
Szulc, P., Schoppet, M., Rachner, T.D., Chapurlat, R., Hofbauer, L.C., 2014. J. Clin. Endocrinol. Metab. 99, 617–624.
PMID: 24276456 -
Terpos, Evangelos, Christoulas, D., Kastritis, E., Katodritou, E., Papatheodorou, A., Pouli, A., Kyrtsonis, M.-C., Michalis, E., Papanikolaou, X., Gkotzamanidou, M., Koulieris, E., Gavriatopoulou, M., Zervas, K., Dimopoulos, M.A., on behalf of the Greek Myeloma Study Group, 2014. American Journal of Hematology 89, 34–40
-
Terpos, E, Christoulas, D., Kastritis, E., Roussou, M., Migkou, M., Eleutherakis-Papaiakovou, E., Gavriatopoulou, M., Gkotzamanidou, M., Kanellias, N., Manios, E., Papadimitriou, C., Dimopoulos, M.A., 2014. Leukemia 28, 928–934
-
Anastasilakis, A.D., Polyzos, S.A., Gkiomisi, A., Bisbinas, I., Gerou, S., Makras, P., 2013. The Journal of Clinical Endocrinology & Metabolism 98, 3206–3212.
-
Brunetti, G., Faienza, M.F., Piacente, L., Ventura, A., Oranger, A., Carbone, C., Benedetto, A.D., Colaianni, G., Gigante, M., Mori, G., Gesualdo, L., Colucci, S., Cavallo, L., Grano, M., 2013. American Journal of Physiology-Endocrinology and Metabolism 304, E546–E554
-
de Rooy, D.P.C., Yeremenko, N.G., Wilson, A.G., Knevel, R., Lindqvist, E., Saxne, T., Krabben, A., Leijsma, M.K., Daha, N.A., Tsonaka, S., Zhernakova, A., Houwing-Duistermaat, J.J., Huizinga, T.W.J., Toes, R.E.M., Baeten, D.L.P., Brouwer, E., van der Helm-van Mil, A.H.M., 2013. Annals of the Rheumatic Diseases 72, 769–775.
-
Gifre, L., Ruiz-Gaspà, S., Monegal, A., Nomdedeu, B., Filella, X., Guañabens, N., Peris, P., 2013. Bone 57, 272–276.
-
Systemic effects of Wnt signaling.
Maruotti, N., Corrado, A., Neve, A., Cantatore, F.P., 2013. J. Cell. Physiol. 228, 1428–1432.
PMID: 23359342
-
Sclerostin and DKK1 in Primary Hyperparathyroidism.
Viapiana, O., Fracassi, E., Troplini, S., Idolazzi, L., Rossini, M., Adami, S., Gatti, D., 2013. Calcified Tissue International 92, 324–329
-
Cejka, D., Jager-Lansky, A., Kieweg, H., Weber, M., Bieglmayer, C., Haider, D.G., Diarra, D., Patsch, J.M., Kainberger, F., Bohle, B., Haas, M., 2012. Nephrology Dialysis Transplantation 27, 226–230
-
Sclerostin and DKK1 in postmenopausal osteoporosis treated with denosumab.
Gatti, D., Viapiana, O., Fracassi, E., Idolazzi, L., Dartizio, C., Povino, M.R., Adami, S., Rossini, M., 2012. Journal of Bone and Mineral Research 27, 2259–2263
-
Gaudio, A., Privitera, F., Battaglia, K., Torrisi, V., Sidoti, M.H., Pulvirenti, I., Canzonieri, E., Tringali, G., Fiore, C.E., 2012. The Journal of Clinical Endocrinology & Metabolism 97, 3744–3750
-
Heiland, G.R., Appel, H., Poddubnyy, D., Zwerina, J., Hueber, A., Haibel, H., Baraliakos, X., Listing, J., Rudwaleit, M., Schett, G., Sieper, J., 2012. Annals of the Rheumatic Diseases 71, 572–574
-
Serum Osteoprotegerin, RANKL, and Dkk-1 Levels in Adults with Langerhans Cell Histiocytosis.
Makras, P., Polyzos, S.A., Anastasilakis, A.D., Terpos, E., Kanakis, G., Schini, M., Papatheodorou, A., Kaltsas, G.A., 2012. The Journal of Clinical Endocrinology & Metabolism 97, E618–E621
-
Polyzos, S.A., Anastasilakis, A.D., Bratengeier, C., Woloszczuk, W., Papatheodorou, A., Terpos, E., 2012. Osteoporos Int 23, 1171–1176.
PMID: 21305266 -
Senolt, L., Hulejova, H., Krystufkova, O., Forejtova, S., Andres Cerezo, L., Gatterova, J., Pavelka, K., Vencovsky, J., 2012. Annals of the Rheumatic Diseases 71, 71–74
-
Taylan, A., Sari, I., Akinci, B., Bilge, S., Kozaci, D., Akar, S., Colak, A., Yalcin, H., Gunay, N., Akkoc, N., 2012. BMC Musculoskelet Disord 13, 191.
PMID: 23025387; PMCID: PMC3492209 -
Voskaridou, E., Christoulas, D., Plata, E., Bratengeier, C., Anastasilakis, A.D., Komninaka, V., Kaliontzi, D., Gkotzamanidou, M., Polyzos, S.A., Dimopoulou, M., Terpos, E., 2012. Horm. Metab. Res. 44, 909–913.
PMID: 22581647 -
Sclerostin and Dickkopf-1 in Renal Osteodystrophy.
Cejka, D., Herberth, J., Branscum, A.J., Fardo, D.W., Monier-Faugere, M.-C., Diarra, D., Haas, M., Malluche, H.H., 2011. Clinical Journal of the American Society of Nephrology 6, 877–882.
-
Feldmann, R., Schierl, M., Fink, A.M., Sator, P.-G., Maiweg, J., Steiner, A., 2011. Dermatology 222, 171–175
-
Frost, M., Andersen, T., Gossiel, F., Hansen, S., Bollerslev, J., van Hul, W., Eastell, R., Kassem, M., Brixen, K., 2011. Journal of Bone and Mineral Research 26, 1721–1728
-
Gatti, D., Viapiana, O., Idolazzi, L., Fracassi, E., Rossini, M., Adami, S., 2011. The Journal of Clinical Endocrinology & Metabolism 96, 1555–1559
-
Ng, A.C., Khosla, S., Charatcharoenwitthaya, N., Kumar, S.K., Achenbach, S.J., Holets, M.F., McCready, L.K., Melton, L.J., Kyle, R.A., Rajkumar, S.V., Drake, M.T., 2011. Blood 118, 6529–6534.
-
Terpos, E., Fragiadaki, K., Konsta, M., Bratengeier, C., Papatheodorou, A., Sfikakis, P.P., 2011. Clin. Exp. Rheumatol. 29, 921–925
PMID: 22032557 -
Voskaridou E., Christoulas D., Papatheodorou A., Bratengeier C., Plata E., Kaliontzi D., Woloszczuk W., Terpos E., 2010. Blood 116:1010
-
Gaudio, A., Pennisi, P., Bratengeier, C., Torrisi, V., Lindner, B., Mangiafico, R.A., Pulvirenti, I., Hawa, G., Tringali, G., Fiore, C.E., 2010. The Journal of Clinical Endocrinology & Metabolism 95, 2248–225
-
Terpos, E., Christoulas, D., Gkotzamanidou, M., Bratengeier, C., Gavriatopoulou, M., Migkou, M., Papatheodorou, A., Kastritis, E., Woloszczuk, W., Dimopoulos, M.A., 2010. Blood 116, 2963–2963
-
Polyzos, S.A., Anastasilakis, A.D., Efstathiadou, Z., Kita, M., Litsas, I., Avramidis, A., Arsos, G., Moralidis, E., Gerou, S., Pavlidou, V., Papatheodorou, A., Terpos, E., 2009. Hormone and Metabolic Research 41, 846–850.
-
Terpos, E., Christoulas, D., Katodritou, E., Bratengeier, C., Lindner, B., Harmelin, S., Hawa, G., Boutsikas, G., Migkou, M., Gavriatopoulou, M., 2009. Blood 114:425;
-
Voorzanger-Rousselot, N, Ben-Tabassi, N.C., Garnero, P., 2009. Annals of the Rheumatic Diseases 68, 1513–1514
-
Voorzanger-Rousselot, Nathalie, Journe, F., Doriath, V., Body, J.-J., Garnero, P., 2009. Calcified Tissue International 84, 348–354
-
Voskaridou, E., Christoulas, D., Xirakia, C., Varvagiannis, K., Boutsikas, G., Bilalis, A., Kastritis, E., Papatheodorou, A., Terpos, E., 2009. Haematologica, 94(5):725-8.
-
Garnero, P., Tabassi, N.C.-B., Voorzanger-Rousselot, N., 2008. The Journal of Rheumatology 35, 2313
-
Glucocorticoids Attenuate the Stimulatory Effect on Bone Formation by Bortezomib.
Lund, T., Søe, K., Abildgaard, N., Garnero, P., Pedersen, P.T., Delaissé, J.-M., Plesner, T., 2008
-
Osteoclasts Are Active in Bone Forming Metastases of Prostate Cancer Patients.
Roato, I., D’Amelio, P., Gorassini, E., Grimaldi, A., Bonello, L., Fiori, C., Delsedime, L., Tizzani, A., De Libero, A., Isaia, G., Ferracini, R., 2008. PLoS ONE 3, e3627.
